Playlist
Show Playlist
Hide Playlist
Hydrocephalus: Diagnosis and Management

-
Slides Hydrocephalus Special Surgery.pdf
-
Download Lecture Overview
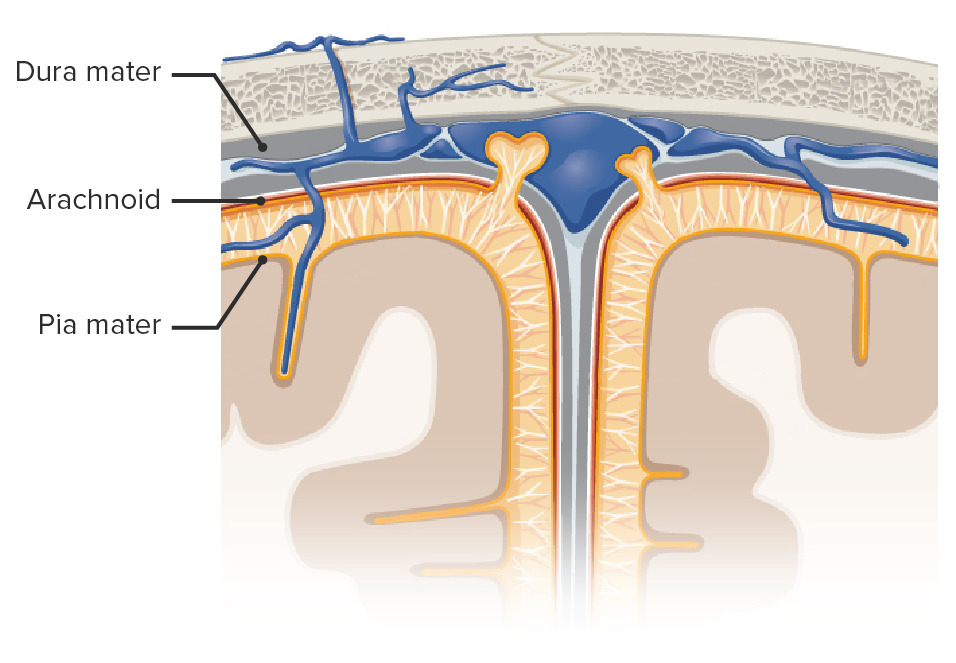
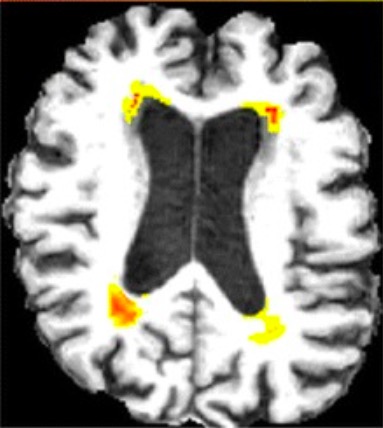
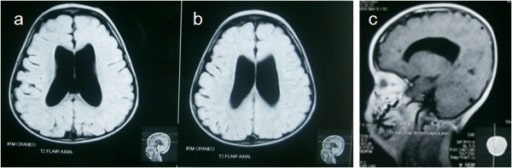
00:01 What about a non-communicating hydrocephalus? This can behave like a mass effect. 00:08 Mass such as a tumor or an extrinsic obstruction of the normal CSF drainage pathway. 00:14 Recall a few slides back, the choroid plexus, all the way to the subarachnoid space, is a defined pathway. 00:21 Any obstruction along that pathway can cause a non-communicating hydrocephalus. 00:26 Remember, the brain has had less time to compensate and more likely to develop intracranial hypertension. 00:34 Besides our physical and history, imaging diagnosis can be helpful. 00:39 Generally speaking, we get a CAT scan. 00:41 The arrow is pointing to you a very decreased amount of lateral ventricle space. 00:47 In this MRI image, you notice quite dilated ventricles. 00:52 This probably represents a CSF accumulation due to the lack of absorption rather than an obstruction. 00:58 Now, you’ve diagnosed hydrocephalus. 01:02 When do we need to treat it? Well, indications for treatment, which includes a ventricular peritoneal shunt, is when the patient becomes symptomatic. 01:11 In this shunt procedure, a catheter is placed between the ventricles, tunneled under the skin and introduced into the abdomen. 01:19 Although a fairly routine procedure, it does contain some complications. 01:23 Mostly, as you can imagine, if the catheter is in the abdomen, intestines can loop around it. 01:28 This catheter can be clogged and becomes dysfunctional. 01:32 It may need to be replaced. 01:34 Additionally, also remember, sometimes the ventricular peritoneal shunt is actually a ventricular plural shunt. 01:41 That's when the ventricular drainage catheter is placed into thoracic – into the thoracic space as opposed into the abdomen. 01:49 Some reasons that neurosurgeons may choose to place it into the thoracic space as opposed to the abdominal space is because of prior surgeries in the abdomen. 01:58 As we previously described, this catheter sits in the ventricle, is tunneled, as you can see in this schematic, either into the thoracic space or into the abdomen. 02:08 Now, it’s time to remind you of some clinical pearls and high-yield information on hydrocephalus. 02:14 Remember the classic findings of normal pressure hydrocephalus? Although rare, it's a popular test question. 02:21 It requires a high index of suspicion, so you as a clinician should think about normal pressure hydrocephalus. 02:28 If the clinical scenario presents with classic findings, you have your answer. 02:34 And remember, Arnold-Chiari syndrome. 02:37 This syndrome is a skull malformation that can cause cerebellar tonsils to displace inferiorly. 02:44 This actually causes an obstruction. 02:46 So, this would not be an example of normal pressure hydrocephalus. 02:50 This is so-called non-communicating hydrocephalus. 02:54 This is high-yield information. 02:56 I’d encourage you to commit it to memory. 02:59 Thank you very much for joining me on this discussion of hydrocephalus.
About the Lecture
The lecture Hydrocephalus: Diagnosis and Management by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
Which of the following can cause CSF obstruction?
- Arnold-Chiari syndrome
- Lou Gehrig's disease
- Brain aneurysm
- Syringomyelia
- Tethered cord syndrome
Which of the following shunts is most frequently used for the management of hydrocephalus?
- Ventriculoperitoneal shunt
- Ventriculopleural shunt
- Ventriculocaval shunt
- Ventriculosubgaleal shunt
- Ventriculogallbladder shunt
Author of lecture Hydrocephalus: Diagnosis and Management

Kevin Pei, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
2 |
| 1 Star |
|
0 |
great lecture. I am now very clear on the differentials. Thanks
Nothing about what to look for on the scan, the exact diagnosis criteria, indicitons for treatment etc.
Very little information is given, I understand lectures need to be easy and contain important information but this is a summary of a summary
