Playlist
Show Playlist
Hide Playlist
HIV in Children: Management & Prevention


-
Slides HIV Pediatrics.pdf
-
Download Lecture Overview
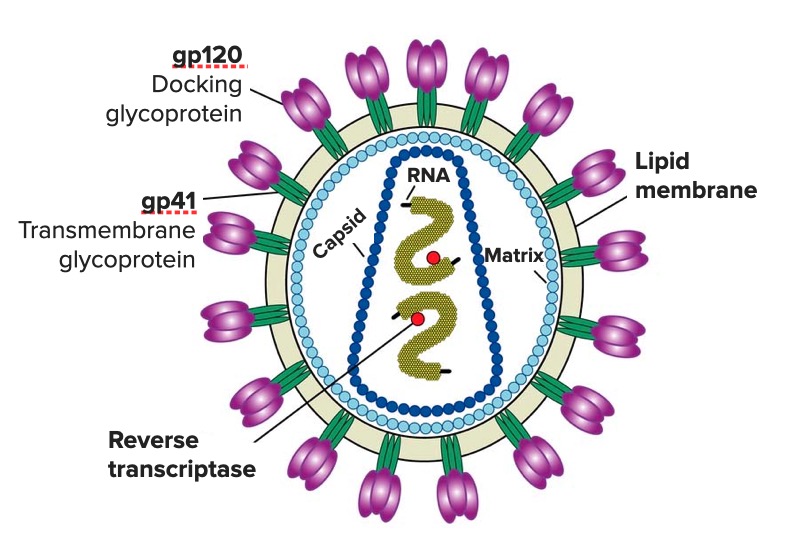
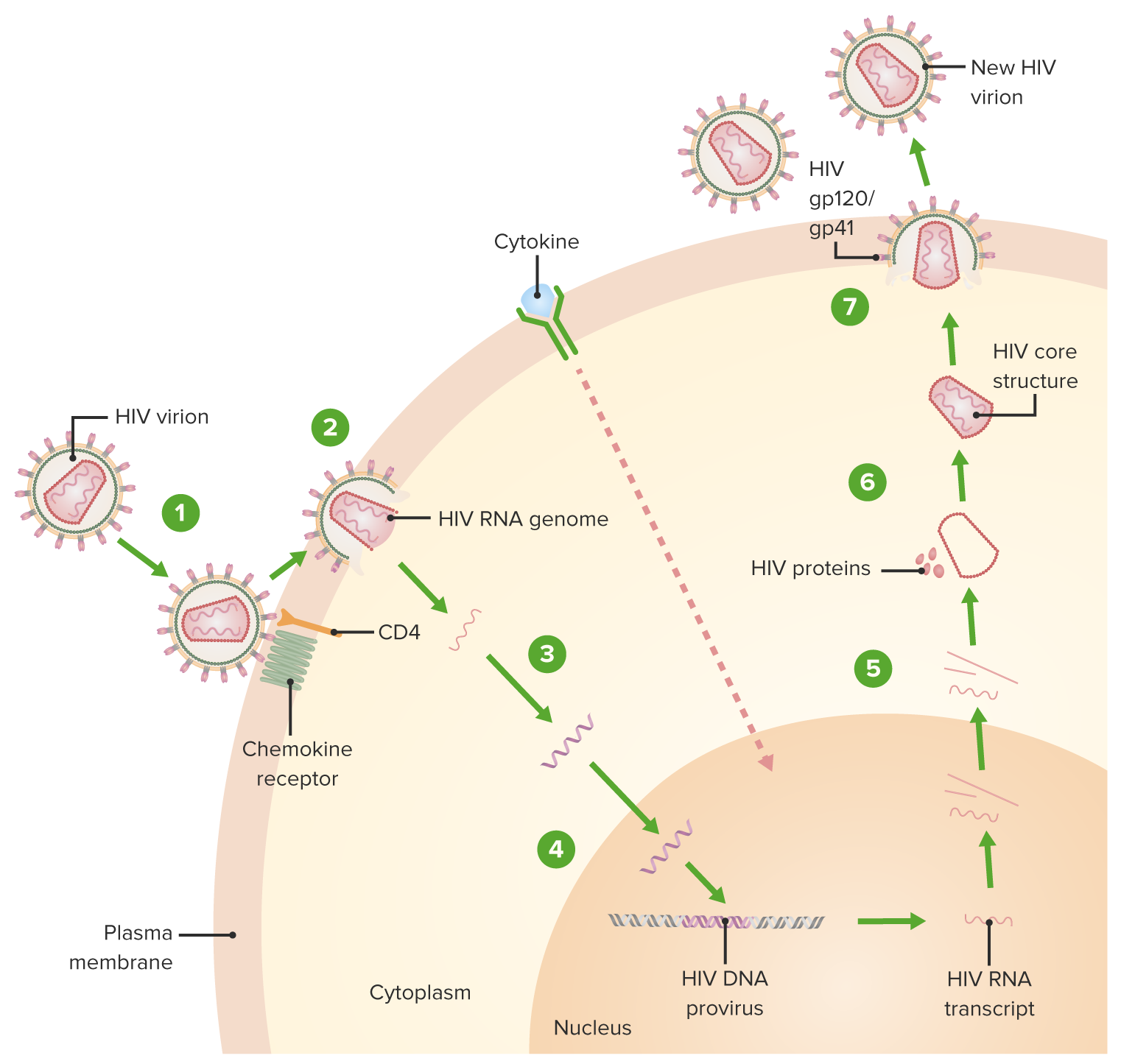
00:00 If we suspect HIV, we should diagnose and treat all the opportunistic infections this patient have. We should generally attempt to use combination antiretroviral therapy, cART or HAART. 00:15 This means that patients will have at least 3 active antiretrovirals from at least 2 different classes of drugs. The reason why we're treating this virus this way is because with just monotherapy, the virus may mutate and become resistant very quickly. Remember, in an actively infected individual, literally billions of copies are being made every day, and the chances of a resistant form are much higher when there’s monotherapy. So, there are many different classes of HIV medication and I want to go through them generally. We have entry inhibitors, fusion inhibitors, non-nucleoside reversed transcriptase inhibitors, nucleoside reverse transcriptase inhibitors, integrase inhibitors, and protease inhibitors. All of these drugs are acting at different stages in viral replication, and you can see here examples of a few that are preventing certain stages of the life cycle of that virus as it grows within the human body. So, let’s go through some disease complications of untreated HIV and treated HIV. So, in untreated HIV, patients can get <i>P. jirovecii</i> which we used to call PCP pneumonia, they may get CMV, HSV, they may get bacterial infections, fungal infections, or often tuberculosis. In treated HIV, we worry about side effects. Examples may be medication side effects, they may have nausea, rash, hypersensitivity reactions, neuropsychiatric symptoms, lipodystrophy may happen as a result of medication side effects and patients may develop resistance to meds leading them back into the untreated category. 02:03 So, the lives of these patients can be quite challenging. With appropriate care, the long-term prognosis in HIV is excellent. It’s not an easy life but right now, life expectancy in the United States is quite good. There are certain things that _____ a better survival rate, and a better life in terms of patients with HIV. Perhaps the most important is earlier detection and treatment. 02:32 If patients are diagnosed early and treated early, they are more likely to be able to live a long and productive life. Patients who have less immunosuppression will generally have better survival likelihood, so that happens earlier in disease. Patients who are compliant with therapy will generally live a long time, and in adolescents it's very hard sometimes to get them on board regarding compliance. So, counseling and discussion with these children are incredibly important. 03:06 The lower your viral load, the more likely your prolonged survival is as well. So, let’s talk about how we prevent HIV. In newborns, it’s better when there are laws in each state that are opt out instead of opt in regarding testing. What this generally means is there are some states in the United States where pregnant mothers are going to get their HIV test and they have to sign a special piece of paper. That’s opt in. In other states, patients come into the hospital to see for their general prenatal care and they are offered HIV testing in the same phrase as they're offered all their other testing that happens during pregnancy. They may choose not to get HIV tested, that is their right, but it’s offered as a result of routine screening. As a result, there is not an extra signature. In states with opt out testing instead of opt in testing, rates of pregnancy testing for HIV are much higher, and if we can test women, they are more likely to know their status at the time of delivery which then prevents transmission of the virus. In a few states such as New York, Illinois, Connecticut, Rhode Island, there is mandated newborn screening as well. This means that testing of the child at the time of birth is mandated if there’s no test for the mother available to the physician. This happens right at birth, and then if the child is positive, HIV care is initiated. In states where this happens, prenatal testing actually goes up much higher. This is probably because in the office setting, the obstetrician says, “We’ll test you for HIV,” and the mother says, “I’m not sure if I want to,” and he says, “Okay, but if you don’t, the baby is going to be tested anyway,” and then almost all mothers will say, “Oh, well in that case, just test me.” This then allows us to really understand exactly what’s going on. We should treat pregnant women to reduce viral load at birth. The treatment of pregnant women dramatically reduces newborn infection rates from 25% to less than 2%. In developing countries where there is more poverty, we tend to recommend continuing breastfeeding. This is because the rate of death from starvation may be higher than the rate of HIV transmission through breastfeeding. Remember, the bulk of vertical transmission is through the birth process, not through breastfeeding. However, in the United States where there are alternatives that are available to poor people such as Wick, we do not recommend breastfeeding in HIV-positive women because in this case, there are easy alternatives for infant nutrition. So, each country has a different approach to whether breastfeeding is recommended depending on the resources available to people regarding formula provision. Now, prevention of HIV in adolescents and adults is a little bit different. For this, we must recommend condom use and we should be providing this advice to all adolescents and adults regardless of their beliefs and circumstances, the availability of condom use is critical to reducing the population burden of HIV. Additionally, we should have routine screening. Again, if a patient is aware of their HIV status, they are much less likely to actually spread the disease. They are more likely to reliably use condoms and they are more likely to not share needles. As such, awareness of your status is critically important. Right now in America, 1 in 4 adults or adolescents with HIV is unaware that they have the disease and those individuals are responsible for more than half of new infections. We can do these things through community outreach programs and that’s what’s important for us to do, for us to fund and have community outreach programs. So, that’s my review of pediatric HIV and HIV in general. 07:21 Thanks for your time.
About the Lecture
The lecture HIV in Children: Management & Prevention by Brian Alverson, MD is from the course Pediatric Infectious Diseases. It contains the following chapters:
- Management of HIV
- Prevention of HIV
Included Quiz Questions
Which of the following is a common presentation of HIV in adolescents that is not seen in infants?
- Flu-like illness during initial infection
- Poor weight gain
- Developmental delay
- Severe thrush
- Bacterial infections
Which test should be ordered in patients who have been diagnosed with pneumocystis jirovecii to rule out HIV?
- PCR
- Western blot
- ELISA
- Rapid viral test
- Fungal staining
Which of the following is NOT a class of drugs used in the treatment of HIV?
- Helicase inhibitors
- Protease inhibitors
- Nucleoside reverse transcriptase inhibitors
- Non-nucleoside reverse transcriptase inhibitors
- Fusion inhibitors
Author of lecture HIV in Children: Management & Prevention

Brian Alverson, MD
Customer reviews
4,7 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
HIV is a topic that is a difficult topic because of the nature of the disease and its consequences. I liked how the topic was delivered and the emphasis on awareness, information and a pragmatic approach.
Very glad to have such succinct and high-yeild lectures. Thanks, Dr. Alverson! I looked like a star during my group session when I brought up that breastfeeding is advised in poverty-stricken areas, but not in countries where programs like WIC make formula feeding affordable.
Sir whats with the new guidelines of HIV AIDS? Have you seen it yet?
