Playlist
Show Playlist
Hide Playlist
Herpex Simplex Virus-1 and Herpes Simplex Virus-2 – Herpesviruses

-
Slides Herpesviridae.pdf
-
Download Lecture Overview
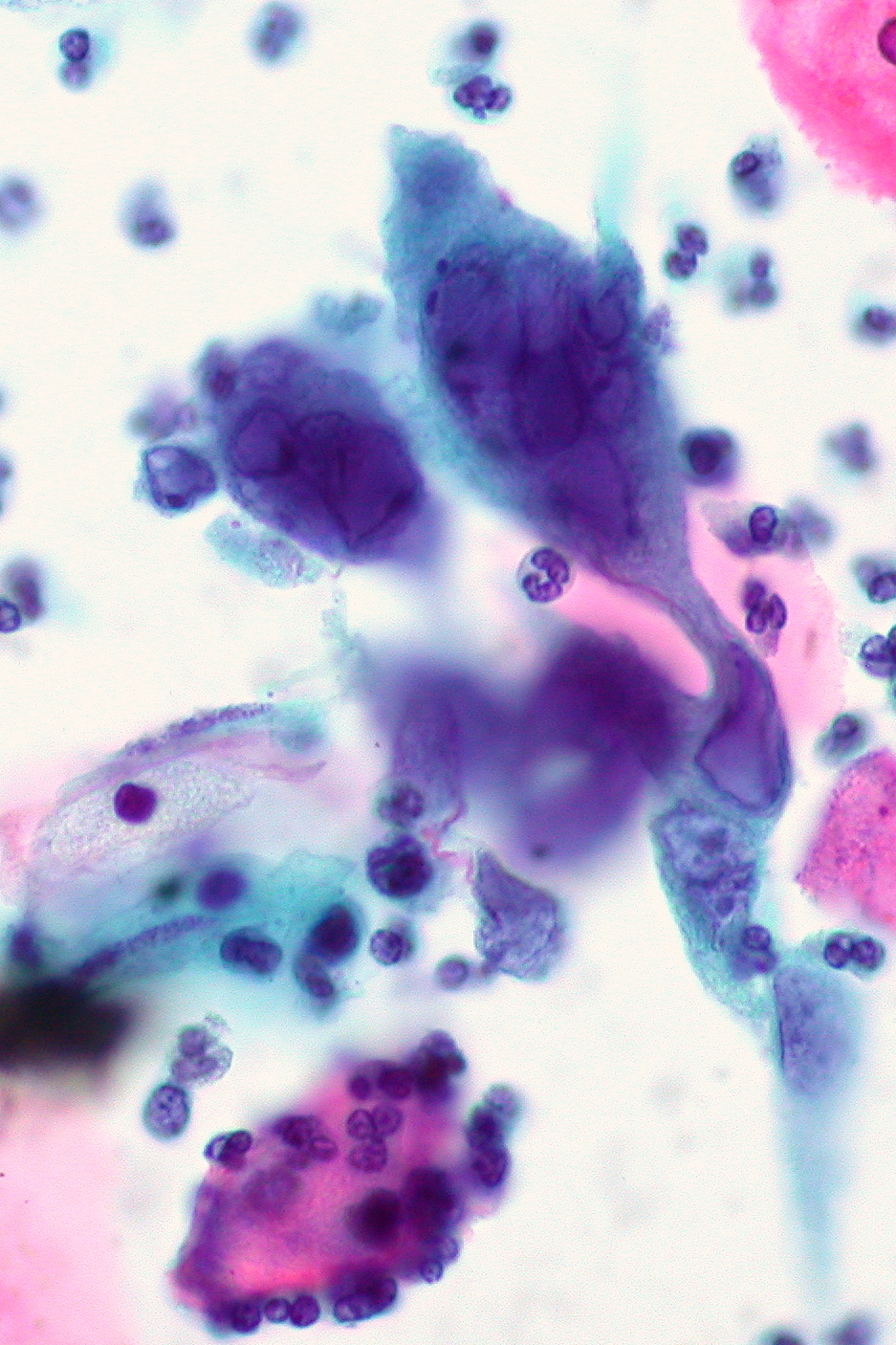
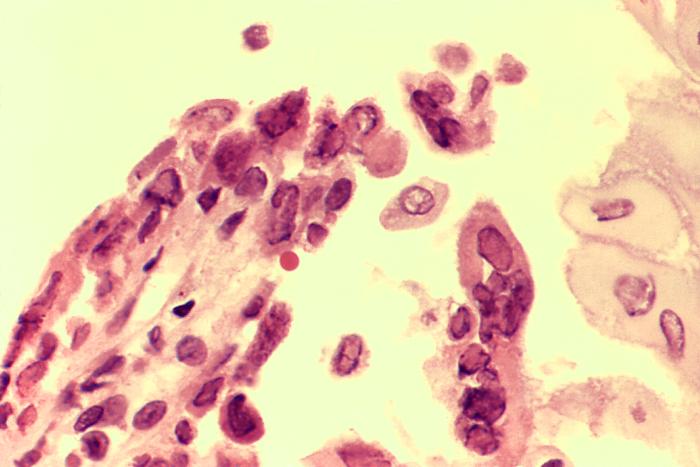
00:01 So let's look now, by pathogenesis, at the first 2 herpesviruses: herpes simplex viruses type 1 and 2. 00:09 These infections occur by initial binding of either herpes simplex virus 1 or 2 to their target mucoepithelial cells. 00:18 And again, depending on whether it's 1 or 2, those typically have tropism for the oral mucosa, conjunctiva mucosa, or the genital mucosa. 00:29 The infections then set up a lytic process. 00:32 Some are going to go become latent, but primarily after the replication process, they create lysis of their target cells, which then causes the inflammatory reaction with all the cytopathic effects, and we get the lesions which we'll look at very shortly. 00:48 The latent infection primarily sets up in a sensory or sensory neural ganglia. 00:53 Keep in mind that herpes simplex types 1 and 2 develop latent infection in neurons. They're neurotropic after their primary infection in the mucoepithelial cells. 01:07 When a patient has some sort of stressor, and this could be physiologic, it could be emotional, there even are some foods in some people, or certainly anybody who is immunosuppressed, then that latent infection within the sensory ganglia can reactivate. 01:23 Reactivation causes a recurrence of the lesions, but in a distribution specific to where the sensory ganglia, which had the latent infection, wherever those might be. 01:35 So, what do lesions look like? Well, the lesions, in general, have erythematous basis. They typically occur 3 days or so after an initial circulation or infection, and they last for up to 2 weeks. 01:49 To identify herpes simplex virus 1 and 2, one can do a Tzanck or Pap smear, but increasingly one uses fluorescent anti- body testing on viral culture specimens. 02:01 One also in pathology can look for syncytia or Cowdry type A inclusion bodies, which you can see as the densely stained bodies toward the top of the slide in front of you. 02:15 Diagnosis of HC infection can be cured in multiple different ways. 02:19 Firstly, one can perform cytology of an active lesion using either a zinc or pap smear. The psychopathic effects seen on these smears would include such things as multi nucleotide giant cells. 02:30 However, these are not very sensitive tests and are definitely technique dependent. 02:34 The most sensitive test and even specific would be polymerase chain reaction PCR, which accurately and sensitively detects the the nuclear material of the viruses themselves. One further can perform biopsy of an active lesion looking for such findings as syncytial cells or nuclear inclusions, and also perform immunohistochemistry on that specimen. 02:56 Direct fluorescent antibody can be formed as can viral culture with a characteristic psychopathic effect and then type specific serologic tests also can be done to distinguish HSV one versus HSV two, especially in patients that may have atypical presentation or to determine whether they have active or old disease. As we see in this slide here, of a biopsy of a herpetic skin lesion stained with HC there are two distinct cytoplasmic effects that one can demonstrate. 03:26 The first in Slide A is epithelial cells with intra nuclear viral inclusions. The second on the right, Slide B demonstrates multi nucleated epithelial cells. 03:37 These are findings typical typically seen in HC infection. 03:44 Transmission of herpes 1. Now, we're looking again specifically at herpes simplex virus 1 which most often is in the, sort of, above the neck region. The transmission is via secretions, so you can imagine through saliva, through kissing, through sneezing, sometimes. 04:02 This virus is everywhere, I'm sorry to say. And in fact, herpes simplex virus type 1 is a very common infection. 04:11 90% of people will be exposed to this virus in childhood. 04:16 Not all develop disease. In fact, very few will develop disease, but it means that all of us might be at risk for having a reactivation with a lovely cold sore later on in life. 04:27 So, when the infection occurs and lysis of the host mucoepithelial cells occurs, then one can see lesions developing in the mouth, or in the finger, or other places, as we'll talk about in just a second. 04:42 The latency, where the virus goes to sleep or hides, is almost always in the trigeminal ganglia. 04:49 That is important because that particular ganglia can also backtrack to the temporal lobe. 04:55 So if you think about neurologic structures, trigeminal, going back to the frontal and temporal lobe is where encephalitis with herpes type 1 occurs. 05:06 It travels backwards to cause a CNS infection. 05:10 So, the diseases that we see with herpes simplex virus type 1 are the herpes labialis, a cold sore, which you can see in the image on the upper part of the slide. 05:21 Very prominent. 05:23 Everybody knows you've got one. They're so common. 05:25 There shouldn't be any shame about it, but of course, all of us try and cover those things up and do topical treatments, etc. 05:33 There also is, along the lines, a gingivostomatitis, which typically is the primary infection, the first mucoepithelial disease. 05:43 And that typically occurs inside the mouth on the gingiva, so the sides of the mouth, the gums themselves, sometimes, the tongue. Very painful, very prominent, but it also can be quite silent as the primary infection. 05:56 One can then self-inoculate to the conjunctiva, causing a keratitis or a uveitis. 06:03 Herpetic whitlow, that is the image on the lower left side of a finger with a white vesicle related. 06:10 That typically comes from inoculation from the mouth to the finger. 06:15 Classically, you'll see this in infants to sometimes toddlers, because an adult -- and it's almost always grandma -- has an active cold sore, and that just has to nibble on those cute little fingers, like those tiny little hangers-on to the fingernails. You've all seen it happen. 06:31 In fact, we've all probably done it. So you just sort of -- nibble on that, and that inoculates herpes from the cold sore active mouth into or on the finger, and then you have secondary infections causing herpetic whitlow. 06:44 The gingivostomatitis, we talked about. 06:47 The encephalitis we've talked about, temporal lobe. 06:50 Typically presenting with confusion, and if you think about your neural mapping, what happens in the temporal lobe? Speech and understanding. So patients will be confused, and they will most likely have an expressive or even a Broca's aphasia. 07:06 They can't get their words out. 07:07 Those would be warning signs, in combination with fever, that the patient has a sporadic or an acquired herpes encephalitis. 07:17 And then finally, erythema multiforme. 07:19 Now, this rash is a reactive or a hypersensitivity rash. 07:24 It is not caused by any viral specific effects, but the body's immune reaction to herpes simplex virus 1 will cause this hypersensitivity rash in many people. 07:36 And keep in mind that that rash, although not pictured here, has flat, erythematous macules, which will have a variable border, the look and different shapes. 07:46 Some might even look a bit targetoid or so. 07:50 And this is an important question to remember for those standardized exams. 07:54 Herpes simplex virus number 1 is the most common cause of erythema multiforme worldwide. Remember that. 08:03 Okay. Herpes simplex virus type 2. 08:05 Now going down to the other part of the body. 08:07 So keeping in mind that this virus mostly has tropism for genital mucoepithelial cells. 08:14 Transmission, therefore, of course is sexual contact, or exposure to the perineal region, therefore, perinatal disease can occur. 08:24 This is slightly less common, although still pretty darn common; 30% in adulthood. 08:30 Important to remember, especially if one is dealing in pediatrics. 08:35 2 studies have shown that women of childbearing age -- and we're talking ages 16 years to 40 years, or so -- were studied to identify how prevalent was herpes simplex virus type 2. 08:48 Both studies were done in the States. 08:51 Both studies show that 28% and 26%, both of them, of women had serologic evidence of having having had herpes simplex virus type 2. 09:04 However, on survey, fewer than half of those positive women knew, remembered that they had had genital herpes. 09:12 So, there is fully a quarter to almost a third of women of childbearing age throughout the world who have had herpes simplex virus 2 as a cause of genital herpes, but not that many women will actually know about it. It was silent. 09:26 They didn't know about it, meaning, they're still at risk for transmitting it to their babies during childhood. 09:33 Mucoepithelial cells in the genital region are the target, and when lysis occurs, one gets lesions such as you see on the picture of the penis in the upper part of the slide. 09:44 Latency occurs in the sacral ganglia, which means that reactivations'll typically occur also in the sacral region, again, most often in the genital mucosa. 09:56 The diseases. Herpes genitalia, or herpes genitalis, will be that primary lytic lesion of the mucoepithelial cells, causing painful, shallow, ulcerated lesions on the genitalia, again, as you see on the picture of the penis at the top. 10:13 Neonatal herpes occurs when the baby is born through the cervix, which itself has lesions. The cervical herpes lesions are typically not painful. 10:24 They're silent. There's not primary nerve fibers at that particular part of the cervix. 10:30 So babies could be born unknowingly to a mother with or reactivated herpes and be exposed to that. 10:37 And then within the first 2 weeks of life, babies may develop skin lesions, such as you see on the infant foot in the lower part of the slide. But most often, look for herpes lesions in neonatal herpes in the scalp, because, why? Well, the scalp was the first thing exposed to the cervix during a normal head-first delivery. 11:00 If the baby also had a scalp electrode, that is a high risk factor for developing neonatal herpes in moms who are herpes-positive themselves. 11:10 And those babies may develop their first herpes lesions right up at the scalp, right where that scalp electrode was. 11:17 Other manifestations of genital herpes can be keratoconjunctivitis, again, through self-inoculation, and then aseptic meningitis. 11:27 Now, this is not the severe encephalitis which we talked about for herpes 1, but an aseptic meningitis, very similar to some other viral infections where there's pain, headache, neck pain, but it goes away on its own after 5 to 7 days.
About the Lecture
The lecture Herpex Simplex Virus-1 and Herpes Simplex Virus-2 – Herpesviruses by Sean Elliott, MD is from the course Viruses.
Included Quiz Questions
In which of the following structures does the latent infection of herpes simplex viruses develop?
- Sensory ganglia
- Sympathetic ganglia
- Parasympathetic ganglia
- Mucoepithelial cells
- Lamina propria
Which of the following part of the human brain is most likely to be involved in sporadic encephalitis caused by herpes simplex virus 1?
- Temporal lobe
- Parietal lobe
- Frontal lobe
- Occipital lobe
- Medulla oblongata
An immune-mediated hypersensitivity rash resulting most commonly from infection by herpes simplex virus 1 is known as which of the following?
- Erythema multiforme
- Erythema marginatum
- Erythema migrans
- Erythema nodosum
- Erythema infectiosum
The causative pathogen of herpes labialis remains dormant in which of the following?
- Trigeminal ganglion
- Petrous ganglion
- Spiral ganglion
- Sacral ganglion
- Geniculate ganglion
Which of the following refers to the typical lesions caused by herpes simplex viruses?
- Vesicles
- Nodules
- Wheals
- Macules
- Plaques
Author of lecture Herpex Simplex Virus-1 and Herpes Simplex Virus-2 – Herpesviruses

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
