Playlist
Show Playlist
Hide Playlist
Herpes Simplex Virus Infection in Darker Skin: Diagnosis and Management

-
Slides Herpes Simplex Virus Infection Diagnosis Management.pdf
-
Download Lecture Overview
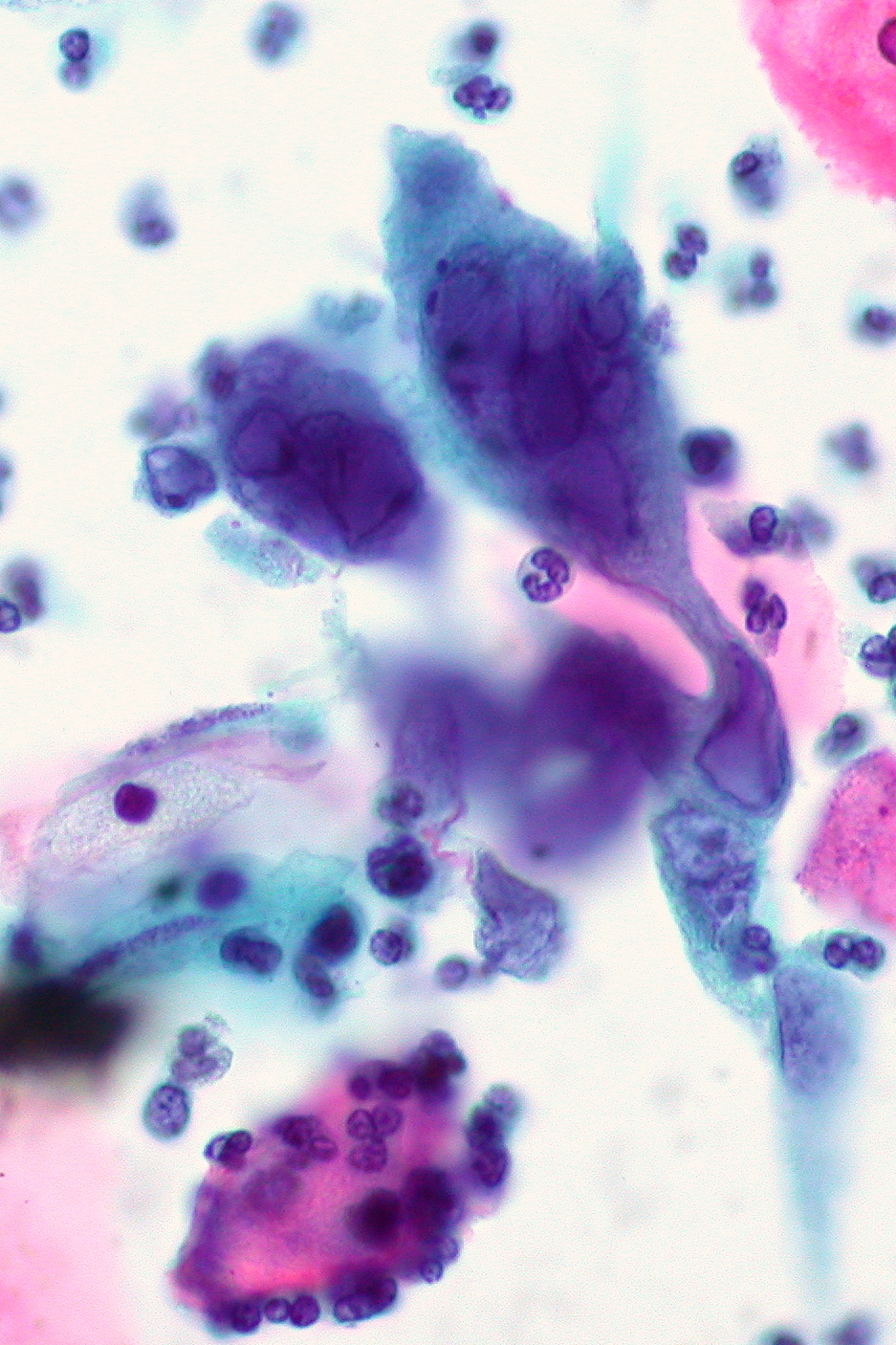
00:01 If one looks at the clinical manifestations, one sees localized pain, tenderness, burning or tingling, which may precede the lesions. Then, painful grouped vesicles appear on an erythematous base. 00:18 Do note, though, that in dark skin, erythema tends to be dusky red or skin colored, depending on the pigmentation of the individual. 00:29 This then progresses to pustules. 00:32 Pustules rupture to form erosions and ulcerations with a characteristic scalloped border. 00:42 Herpes labialis is the most common manifestation of recurrent HSV-1 infection. It's also known as cold sores. 00:50 The classical hepatic lesion is preceded by the prodrome of pain, burning and tingling, so you can see the grouped vesicles on that picture with an erythematous base. 01:01 But do remember that in dark skin this may be more dusky or skin colored. 01:06 Eczema herpeticum is an extensive cutaneous vesicular eruption that arises from preexisting skin disease, most common with atopic dermatitis and sometimes seborrheic dermatitis. 01:20 There is a higher risk in children you can see in this picture. 01:25 Patches of atopic eczema in the background and isolated lesions of vesicles, that is, secondary infection with herpes virus infection, which we call eczema herpeticum. 01:39 Genital herpes. Most genital acquisitions occur in more than 85%, and they are due to oral to genital transmission through oral sex. The classical herpetic lesions with additional features such as dysuria and mucous discharge are seen in patients with genital herpes. 02:02 So you can see on the left genital herpes in males isolated vesicles. Some of them are denuded because the roof has been removed spontaneously. 02:16 On the right hand side, you can see the female genital area and genital herpes with grouped lesions just below the clitoris. One can also see lesions around the anus, and these are grouped painful lesions depending on the mode of sexual contact. 02:41 Hepatic proctitis is seen in persons that engage in anal intercourse. So we need to remember to examine and ask patients about these as well. 02:55 The complications of herpes simplex virus infection are usually seen in immunocompromised patients, and one can get encephalitis and Bell palsy, as you can see on this picture. 03:09 One can also see hepatitis as a complication of HSV infection. The diagnosis of HSV is usually clinical, and of course physical examination may also assist. Laboratory studies include culture, which is viral culture, and PCR, which is more sensitive than viral culture. 03:34 Antibody testing using zinc smear and direct fluorescent antibodies are less sensitive and less specific. 03:45 So what is the differential diagnosis of oral herpes? Oral candida can be easily confused with oral herpes, but it tends to be more superficial and the lesions are pustules rather than vesicles. 03:58 Herpes zoster. In herpes zoster, you see vesicles and pustules, which are usually arranged in a dermatomal pattern following the dermatome, and usually appear for the first time in older individuals or those who are infected with HIV or those patients on chemotherapy for cancer. 04:18 We've just looked at oral herpes and its differential. 04:21 Now we want to speak about genital herpes and its differentials. 04:26 The main primary differential for genital herpes is primary syphilis. 04:31 This is a painless, indurated clean based ulcer, which is called a chancre, which we spoke about in our lectures. 04:39 The next differential is the chancroid. 04:41 This lesion is deep undermined purulent ulcer that may be associated with painful inguinal lymphadenitis. 04:51 So how do we manage these patients? We use antivirals oral or intravenous , as well as topical. The therapy helps to reduce the duration of illness by more than 50% . For frequent and recurrent severe relapses, you may consider prophylactic antivirals.
About the Lecture
The lecture Herpes Simplex Virus Infection in Darker Skin: Diagnosis and Management by Ncoza Dlova is from the course Viral Skin Infections in Patients with Darker Skin.
Included Quiz Questions
What is the typical progression of herpes simplex virus lesions after the prodromal phase?
- Grouped vesicles on an erythematous base → pustules → erosions and ulcerations with scalloped borders
- Papules → plaques → scales → hyperpigmentation
- Macules → wheals → bullae → crusts
- Nodules → abscesses → sinus tracts → scarring
- Petechiae → purpura → ecchymosis → necrosis
Which preexisting skin condition is most commonly associated with the development of eczema herpeticum?
- Atopic dermatitis
- Psoriasis
- Rosacea
- Acne vulgaris
- Lichen planus
What is the key feature that differentiates primary syphilis from genital herpes?
- Primary syphilis presents as a painless, indurated clean-based ulcer (chancre)
- Primary syphilis always presents with multiple vesicles in a dermatomal pattern
- Primary syphilis causes severe dysuria and mucous discharge
- Primary syphilis lesions are always associated with fever and malaise
- Primary syphilis presents with deep, undermined purulent ulcers
Author of lecture Herpes Simplex Virus Infection in Darker Skin: Diagnosis and Management

Ncoza Dlova
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
