Playlist
Show Playlist
Hide Playlist
Hepatocellular Carcinoma (HCC) with Case

-
Slides Gastroenterology 17 Hepatobiliary Malignancy.pdf
-
Reference List Gastroenterology.pdf
-
Download Lecture Overview
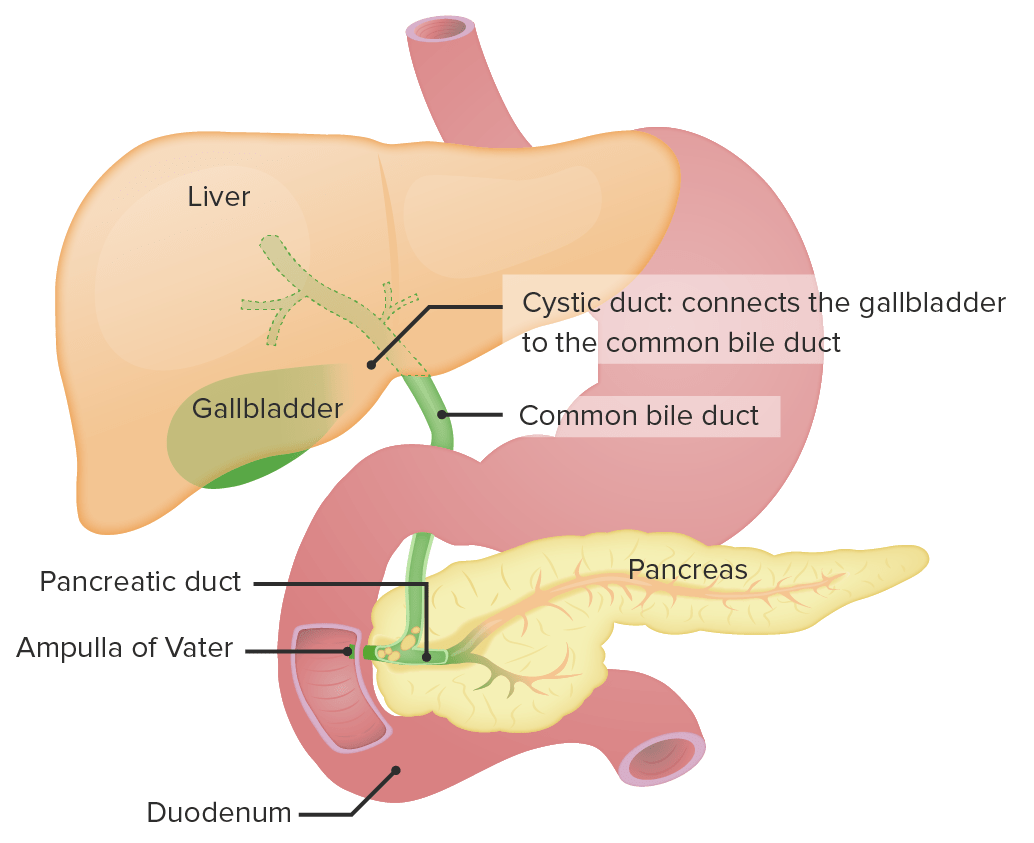
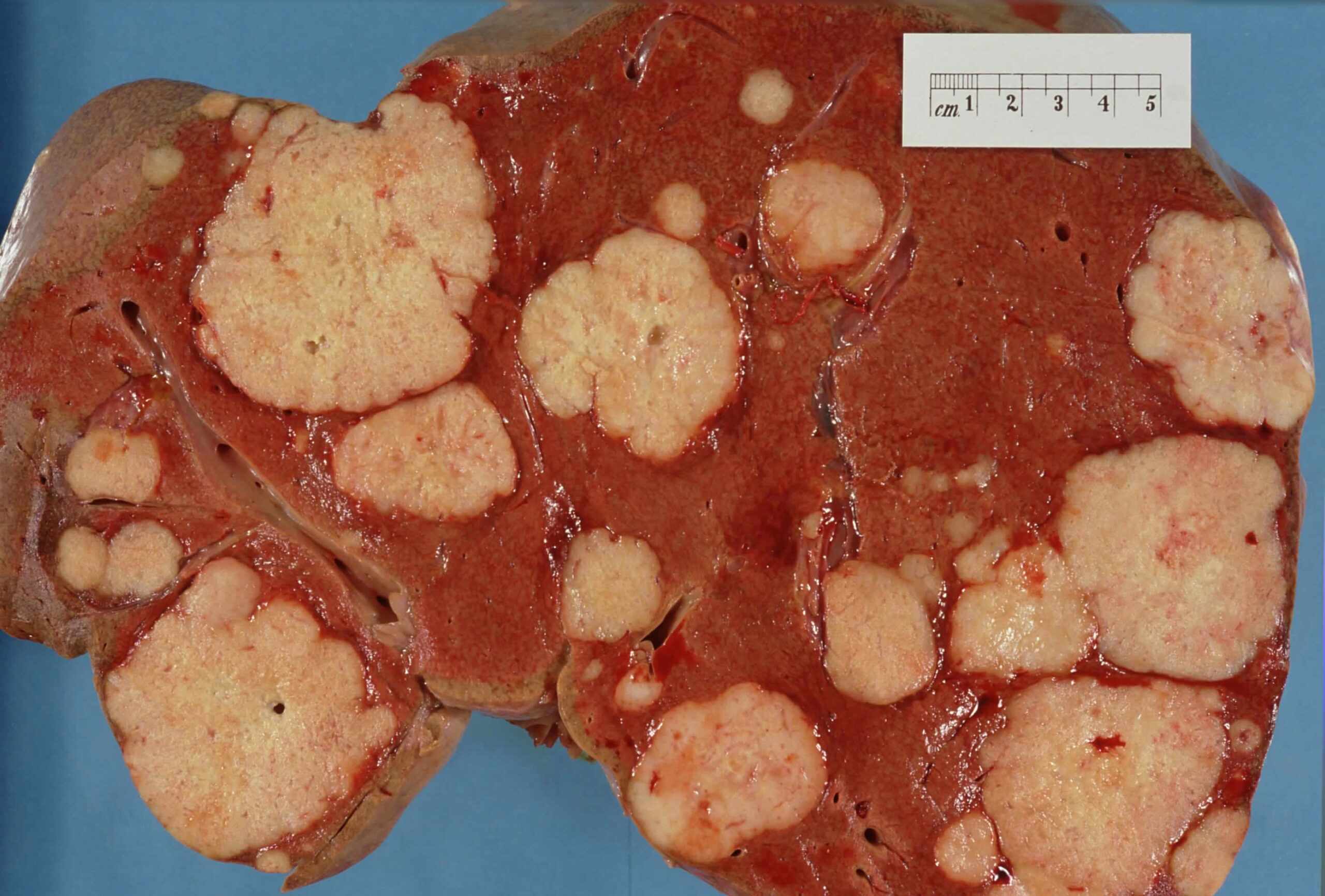
00:00 Welcome. 00:01 Today we'll talk about malignancies of the hepatobiliary system. 00:07 So we'll begin with a case. 00:08 A 45-year-old man with chronic hepatitis B presents to clinic for a routine follow up. 00:15 He was adopted from China and has been diagnosed with hepatitis B as an infant. 00:20 Since then, he has been on Tenofivir without issues. 00:24 He has been feeling well without any new symptoms. 00:27 Vitals are normal , his abdominal exam is benign. 00:30 He has no ascites, jaundice, scleral icterus or hepatomegaly. 00:35 A screening ultrasound last month, showed two new liver masses. 00:40 A follow-up triple-phase CT scan showed two lesions both less than 2 cm in size with arterial enhancement and venous washout. 00:50 What is the most likely diagnosis? So before we answer that question, let's look at some key items in this case. 00:57 He has a history of chronic hepatitis B from vertical transmission and he is from a region where hepatitis B is known to be endemic. 01:07 He has no signs of cirrhosis on exam. 01:11 And his imaging is concerning for potentially a malignancy although at this point, we don't know whether it's a primary liver tumor or metastasis to the liver. 01:22 In addition, there is this added feature of having arterial enhancement with venous washout, we'll talk about what that means in a bit. 01:32 So let's now speak about hepatocellular carcinoma, or HCC. 01:38 Most cases, around 80% will arise in the context of cirrhosis, so recall that with chronic inflammation, you can eventually lead to permanent scarring of the liver with the cirrhosis and this predisposes people to then develop HCC The highest incidence of HCC can be found in regions in Africa, China, Taiwan and Hongkong. 02:01 Symptoms include abdominal pain, weight loss, loss of appetite or anorexia and fatigue The diagnosis can be confirmed by imaging alone. 02:13 So you may do triple-phase CT scan, which we'll discuss a bit later. 02:17 You may also do a contrast-enhanced MRI. 02:21 And only for equivocal cases, when the diagnosis is unclear, you may need to do a liver biopsy. 02:29 So, what is a triple-phase CT scan? This refers to three phases: arterial, portal venous and delayed phases of contrast So we take images of the liver on CT at specific times after giving contrast intravenously. 02:47 HCC has a particular appearance on a triple-phase CT scan. 02:52 So, on the left side, you see two masses within the liver that are showing arterial enhancement, meaning they are brighter than the rest of the tissue surrounding them. 03:04 In panel B, on the right side, you see now venous phase washout. 03:09 So this is when we time the CT, at some point after the IV contrast is given, when the contrast is beginning to wash out in the veins so now you can see those two masses that used to be bright are now darker in color than the rest of the liver parenchyma around them. 03:26 And this is what's called, typical appearance of HCC with arterial enhancement and venous phase washout. 03:33 As a quick high-yield aside, remember that hepatitis B is the one infection that can cause hepatocellular carcinoma without first progressing to cirrhosis So with hepatocellular carcinoma, the key thing is to prevent this diagnosis. 03:50 So to that end, we screen all patients with cirrhosis with a liver ultrasound every 6 months to look for HCC. 03:58 Keep in mind also that those patients who have hepatitis B can develop HCC without cirrhosis so all patients with hepatitis B should also be screened at the same frequency. 04:10 Here, you can see an example of a liver ultrasound and if you look closely at the image towards the top, there is a well-circumscribed circular lesion that is concerning potentially for HCC. 04:23 The treatment options, like with most cancers depends greatly on the size and the number of lesions. 04:31 So your options include first, surgical resection that can be done for small lesions, and in patients who don't have decompensated cirrhosis. 04:42 There are other non-surgical options including transarterial chemoembolization or TACE for short. 04:49 This involves injecting chemical material directly into the arteries that are supplying the HCC mass and thereby cutting off the blood supply and shrinking the tumor. 05:01 Another method we can do is called radiofrequency ablation or RFA. 05:07 This is done for larger lesions or when patients have multiple lesions. 05:12 There are many other methods of non-surgical treatment for tumors that are confined to the liver but too large to be resected. 05:20 These methods include stereotactic body radiation therapy or SBRT, and multiple other methods of locoregional techniques that may use microwave radiation, laser ablation, cryoablation, or ultrasound ablation. Details about these techniques are beyond the scope of this lecture. 05:39 There are also medications like Sorafinib that targets the angiogenesis or the growth of blood vessels that are supplying the HCC tumor. 05:49 This is particularly used for very vascular tumors or if they have extrahepatic spread of the tumor in the context of cirrhosis. 06:00 Lastly, liver transplantation can be an option for select patients with HCC. 06:09 So, who gets referred for liver transplantation? Why not transplant everyone who has hepatocellular cancer? The answer is quite complicated and it depends on several criteria. 06:20 One of the systems we use is the Milan criteria. 06:24 So, this is a system that has been devised to show that those who have a tumor up to 3 tumors all less than 3 cm or 1 tumor less than 5 cm without any invasion of the tumor into the vascular structures or outside of the liver. 06:42 We know that these people have an excellent 5-year prognosis. 06:46 So, these are the people that we can refer for liver transplantation evaluation. 06:53 So now we can return to our case. 06:55 Our 45-year-old man with a history of chronic hepatitis B from vertical transmission. 07:00 He luckily has no signs of cirrhosis on exam, although, since he has hepatitis B, he may still have cancer. 07:07 And his imaging findings are concerning for cancer. 07:11 The answer really comes from the last part of the case that tells you that it appears to be arterially enhancing with venous washout. 07:19 So the most likely diagnosis is hepatocellular carcinoma. 07:24 You should always suspect this diagnosis in anyone with a chronic hepatitis with a new liver mass. 07:30 What really clinches the diagnosis here is the typical appearance of arterial enhancement with venous phase washout and thus you do not need to do a biopsy.
About the Lecture
The lecture Hepatocellular Carcinoma (HCC) with Case by Kelley Chuang, MD is from the course Disorders of the Hepatobiliary Tract.
Included Quiz Questions
Which of the following viruses can cause HCC in the absence of cirrhosis?
- Hepatitis B virus
- Hepatitis C virus
- Hepatitis A virus
- Hepatitis E virus
- Hepatitis D virus
How often should screening ultrasonography be done in patients with hepatitis B virus infection without concurrent cirrhosis?
- Every 6 months
- Every 12 months
- Every 3 months
- Every 2 months
- Every 2 years
Which of the following is part of the Milan criteria for liver transplantation in patients with HCC?
- Up to 3 tumors, all <3 cm
- Up to 3 tumors, all >3 cm
- 1 tumor <5 cm with an extrahepatic spread
- 1 tumor <5 cm with vascular invasion
- 1 tumor >5 cm with no vascular invasion
Which of the following is the treatment of choice for HCC with vascular invasion and extrahepatic spread?
- Sorafenib
- Surgical resection
- TACE
- Liver transplantation
- RFA
Author of lecture Hepatocellular Carcinoma (HCC) with Case

Kelley Chuang, MD
Customer reviews
3,7 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
Very concise and High-Yield. Everything is written on the slides, so need to take notes.
excellent lecture. good amount of detail. high yeild. thank you
90 percent of the stuff she says is written on the lecture , she does not add anything to it , does not explain anything . The lectures are very simple and not in detail , not good for med students
