Playlist
Show Playlist
Hide Playlist
Hematology: Pharmacology

-
Slides Hematology-Pharmacology.pdf
-
Download Lecture Overview
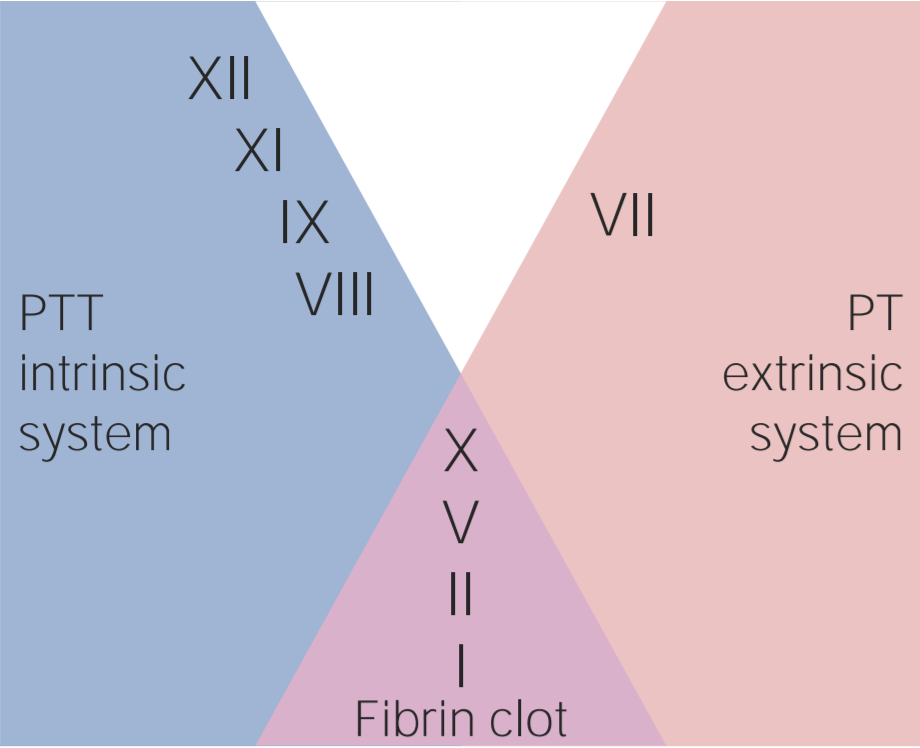
00:01 Welcome back! We'll take a look at hematology and its management but this will be in a form of what we need to do so we can break up a thrombi and to begin by looking at our first drug, heparin. 00:14 So what is heparin? Well, "heparin, we" earlier we had a discussion where we introduced a concept of coagulation cascade, both the intrinsic and extrinsic, please picture that for me. 00:25 Next, if you're thinking about heparin then you automatically reflexively that we should be going to the intrinsic pathway and with the intrinsic pathway you do remember that you can start your intrinsic pathway with a factor called XII or Hageman factor and also we went on to talk about how the intrinsic pathway you would be able to follow. 00:45 Lab wise, like following PTT which is a time of 25 to 40 seconds. 00:52 During the discussion we also introduced a factor called Factor II which is prothrombin. 00:58 So here we are in a situation, let's say that the patient is a lady and she's pregnant, she has too much estrogen. 01:06 Maybe she's non-ambulatory because she is post surgery or anyone for that matter, post surgery, non-ambulatory. 01:13 Maybe the patient is obese, maybe a smoker, so on and so forth so I'm giving all the risk factors of developing a DVT, correct? Well, there you have it and in a patient who's developed a DVT, obviously, worried about embolization and with embolization you're worried about it going straight into the pulmonary vasculature resulting in a PE, obviously, and still a big issue isn't it, clinically? And so at this point you have such a suspicion so therefore you wanna break up the thrombi rather quickly and you will quickly break it up by using heparin. 01:46 So what is heparin? It's a cofactor of antithrombin. 01:50 There it is, there is no factor II and we're gonna now antagonize it. 01:56 So not only are you going to antagonize your thrombin but you may also antagonize Factor X and so by doing so what have you done in a very quick fashion within seconds, literally, you've then caused your breakup of a DVT. 02:09 Now, is it only for DVT that you may use it for? No, well, honestly you could use it for thrombi formation in conjunction with other antithrombotics on the arterial side such as aspirin, maybe clopidogrel that we'll talk about in a bit and so therefore, what I would like for you to do is once again divide your thrombi into arterial thrombi and venous thrombi for organization purposes, right? And so down the arterial side, maybe of acute coronary syndrome and by that we mean maybe unstable angina or prinzmetal angina or maybe patient has even suffered a myocardial infarction. 02:45 And in addition to giving your thrombolytics on the arterial side, maybe you wanna give this patient heparin. 02:52 You're doing everything in your power to then destroy this clot. 02:55 Now as I told you earlier as well heparin is a drug that is not teratogenic and so therefore can be used during pregnancy because it doesn't cross the blood-brain barrier and as I said, we follow the PTT here for heparin. 03:09 There's a particular derivative of heparin or heparin-like and that's called fondaparinux. 03:17 From now on, let me make your life easier, anytime that you see a letter x in a drug such as apixaban or rivaroxaban or fondaparinux and each one of those are a little bit different but ultimately, whenever you see the letter x, whenever you're doing a clinical scenario, you should be thinking about that drug inhibiting factor X only. 03:40 Only. 03:41 Factor X only. 03:42 This is heparin. 03:43 Works not only on thrombin but also on factor X, whether you have a drug called fondaparinux which would work exclusively on factor X. 03:51 And the toxicity has the following. 03:53 There was a situation that I had discussed earlier where you could develop necrosis not only with heparin but also with warfarin, but the occasion of the necrosis would be different. 04:05 For example, if it's heparin then you must give this either your IV or perhaps subcutaneous and at the site of injection you made them cause activation of platelet factor IV and when you do you made them bring about a condition called heparin induced thrombocytopenia. 04:21 In other words, because of rapid thrombi formation that may take place in a sub-set of population, you make them cause a decrease in platelet count resulting in thrombocytopenia that of course would cause a increase in bleeding time if you remember. 04:33 Now in addition to that, what else could you do? Well, in a little bit I'm gonna discuss with you other drugs that also could work directly inhibiting thrombin and those would then include drugs such as dabigatran. 04:47 Now dabigatran, in the family, would be the only one in which it would be the only oral anticoagulant that is a direct acting thrombin inhibitor if the patient perhaps is suffering from HIT, in other words heparin induced thrombocytopenia. 05:02 Keep that in mind please. 05:02 And now, what are the things that you're paying attention to? You do have lower weight type of heparin and this includes enoxaparin and that's a little bit more better in terms of bioavailability. 05:16 And then we just talked about the clinical correlation with heparin induced thrombocytopenia where, as I said, in a sub-set of population an autoantibody then cause activation of a platelet via platelet factor IV and by doing so you are in a state of hypercoagulability which is not what you're looking for in a patient that will came in with a thrombophilia type of situation such as a DVT. 05:45 Keep that in mind. 05:46 And as a derivative or as an alternative to heparin, maybe using a direct acting thrombin inhibitor such as dabigatran.
About the Lecture
The lecture Hematology: Pharmacology by Carlo Raj, MD is from the course Hemostasis: Basic Principles with Carlo Raj.
Included Quiz Questions
What is the normal range of partial thromboplastin time?
- 25-40 seconds
- 15-20 seconds
- 40-60 seconds
- 50-65 seconds
- 45-90 seconds
Which of the following does NOT increase the risk of deep venous thrombosis?
- Weight loss
- Surgery
- Obesity
- Pregnancy
- Smoking
Which of the following laboratory tests is typically used to monitor the activity of unfractionated heparin?
- Partial thromboplastin time
- Prothrombin time
- International normalized ratio
- Bleeding Time
- Clotting time
Protamine sulfate antagonises the effect of unfractionated heparin because of which of the following properties of heparin?
- Strong negative charge
- Solubility of heparin
- Strong positive charge
- Neutrality of heparin
- Acidity of heparin
Author of lecture Hematology: Pharmacology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
heparin...heparin heparin...thats what u wanted... ;)...thanx 4 all the knowledge we need on heparin...and great great quiz questions.....
1 customer review without text
1 user review without text
