Playlist
Show Playlist
Hide Playlist
Granulomatosis with Polyangiitis and Goodpasture Syndrome


-
Slides WegenersandGoodpastures Pediatrics.pdf
-
Download Lecture Overview
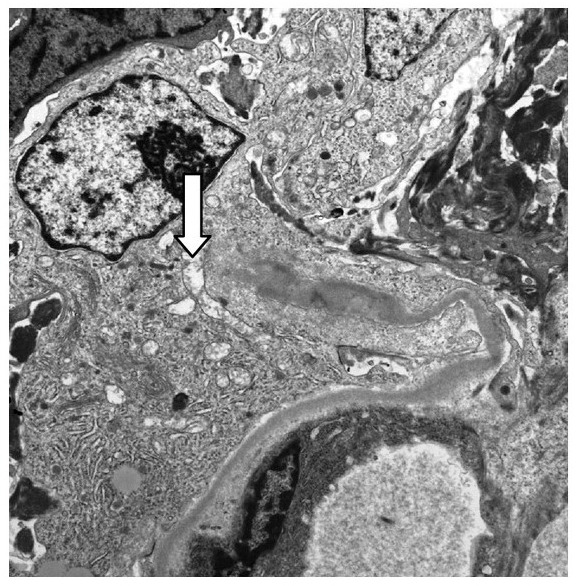
00:01 In this lecture, we will discuss granulomatosis with polyangiitis which used to be called Wegener's syndrome and Goodpasture syndrome. These are both rheumatologic conditions that affect both the kidneys and the lungs. So, let’s start with granulomatosis with polyangiitis. 00:22 This is an autoimmune vasculitis. It primarily affects medium-sized blood vessels of both the lungs and the kidneys. It’s a rare condition. I’ve only made this diagnosis once in children. 00:36 So, there are constitutional, pulmonary, and renal symptoms that I’d like to cover. First, constitutional, these patients may have fatigue, fever, malaise. They may develop anorexia or weight loss like any other autoimmune condition. These patients will have pulmonary symptoms. They focus primarily around the pulmonary hemorrhage. These patients will be found to be coughing up blood. 01:03 Any time a child is coughing up blood, you know something is very wrong. This is one of those conditions that can cause it. Their cough will be bloody. On X-ray, you may see pulmonary nodules. 01:15 Those pulmonary nodules are commonly seen in this disease. Additionally, patients will have renal findings and in particular, hematuria. So, they’ll be coughing up blood and they’ll be peeing out blood. They may also have proteinuria as well. This renal disease can result in hypertension and renal failure. In addition to these classic findings, there are a few other findings you should know about. 01:44 These patients may have chronic otitis media. They may get destruction of the cartilage of the nose resulting in a saddle nose deformity. Those might show up on your exam. So, let’s talk about testing for this disease. The hallmark test for a patient where you suspect granulomatosis with polyangiitis is the c-ANCA. Of course, they may have other findings too like elevated inflammatory markers or urine and blood on the urinalysis or nodules on their chest X-ray. But the c-ANCA is positive in more than 80% of these patients. Let’s pause for a moment and remember what ANCA is. 02:27 ANCA is an antinuclear antigen, which antibody, which is found in neutrophils and monocytes in patients with autoimmune vasculitis. When we look for this antibody, we may see it in the cytoplasm which is a c-ANCA or in a perinuclear pattern which is a p-ANCA. You can see that the cytoplasm in the p-ANCA positive patient is not lighting up and the perinuclear region is not lighting up in the c-ANCA positive patient. c-ANCA is classically seen in Wegener's. p-Anca is seen in other autoimmune conditions. So, let’s look at these two. c-ANCA is classic in inflammatory bowel disease. 03:15 It may be seen in primary sclerosing cholangitis or it can be seen in granulomatosis with polyangiitis or cystic fibrosis. 03:25 Likewise, the p-ANCA is sometimes seen in IBD, is seen in drug vasculitis, and may be seen in autoimmune hepatitis. So basically, when we see these patterns, there are certain diseases that tend to fit in one or the other or perhaps both conditions like inflammatory bowel disease. 03:45 So, let’s shift gears now to Goodpasture syndrome which is also an autoimmune disease that affects the lungs and the kidney. 03:56 In this case, the antibodies are directed against basement membrane proteins. 04:01 These antibodies cause inflammation along those basement membranes, and that in turn is primarily found in both lung and kidney. So these patients, just like patients with polyangiitis are going to have a constitutional, a pulmonary, and a renal finding. Their constitutional symptoms are usually fever and malaise. 04:27 Their pulmonary symptoms include cough, again hemoptysis, and again respiratory distress. 04:33 Their renal findings are more likely to be proteinuria with generalized edema or hypertension resulting. 04:42 So, in patients with Goodpasture syndrome, we are going to do serum testing for the anti-glomerular basement membrane auto antibody. So basically, it’s looking for antibodies that are bound to the basement membrane. In patients who end up with a renal biopsy for what is presumed to be nephrotic syndrome, we may pick up the evidence of Goodpasture syndrome. Basically on biopsy, anti-GBM antibodies will show up with a linear deposition on immunofluorescent staining. 05:15 Here, you can see such a case. This is a glomerulus that is lighting up with the basement membrane being the target of this antibody response. 05:25 The treatment of Goodpasture is important because these patients can get very sick. We usually start with steroids as a way of controlling the autoimmune response. Patients may end up on cyclophosphamide and may benefit from rituximab. We will do plasmapheresis for any patient who has hematemesis or a non-responsive renal disease. Those patients have the worst prognosis. So, that’s my brief summary of these two diseases that are autoimmune affecting the lung We usually start with steroids as a way of controlling the autoimmune response. 05:37 Patients may end up on cyclophosphamide and may benefit from rituximab. We will do plasmapheresis for any patient who has hematemesis or a non-responsive renal disease. Those patients have the worst prognosis. 05:52 So, that’s my brief summary of these two diseases that are autoimmune affecting the lungs and the kidneys Sometimes people get confused. I’m hoping that by presenting them side by side, you can see these key differences. 06:06 Thanks for your time.
About the Lecture
The lecture Granulomatosis with Polyangiitis and Goodpasture Syndrome by Brian Alverson, MD is from the course Pediatric Rheumatology and Orthopedics. It contains the following chapters:
- Granulomatosis with Polyangiitis
- Goodpasture
Included Quiz Questions
Which of the following diseases features p-ANCA positivity?
- Autoimmune hepatitis
- Rheumatoid arthritis
- Cystic fibrosis
- Biliary obstruction
- Multiple myeloma
Which of the following is NOT a feature of Granulomatosis with polyangiitis?
- Hepatic nodules
- Pulmonary hemorrhage
- Weight loss
- Hematuria
- Hypertension
Which statement is INCORRECT regarding Granulomatosis with polyangiitis?
- It primarily affects the heart and genitourinary tract
- It is an autoimmune vasculitis.
- Patients often present with fever, malaise, and fatigue.
- It is c-ANCA positive.
In Goodpasture syndrome, what are antibodies directed against?
- The proteins of the glomerular basement membrane
- IgGs
- Monocytes
- Smooth muscle cells
- Myocardium muscle cells
Which of the following is the first therapeutic agent used in Goodpasture syndrome?
- Steroids
- Cyclophosphamide
- Rituximab
- Plasmapheresis
- NSAIDs
Author of lecture Granulomatosis with Polyangiitis and Goodpasture Syndrome

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I like the clear explanation and breakdown of the topics. I think the other lecture for Granulomatosis with polyangiitis is a little more specific, like chronic sinusitis and pneumonitis +/- cavitary lesions.
To answer your question: yes it is very helpful to see them side by side. Once more it would have been great to have you as our teachers' teacher. Thanks!
