Playlist
Show Playlist
Hide Playlist
Fungal and Cryptococcus

-
Slides 10 CNSInfections Neuropathology I.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
00:01 We're going to move into fungal now. 00:03 Are you ready? Fungal. 00:05 So let’s talk about this fungal meningoencephalitis. 00:09 So here, we’ll get into an interesting dynamic, right? We have meninges. 00:14 And what does encephalitis mean to you? Good. 00:17 Brain parenchyma. 00:18 Now, your most common patient who is susceptible to fungal as you’d expect anywhere up and down the body would be in an immunocompromised patient, right? For example, what if you have fungal infection of the esophagus? Boy, immunocompromised. 00:35 What if you find oral thrush? You take a tongue depressor and you scrape of the white stuff off the tongue. 00:42 Immunocompromised is what you’re thinking already. 00:45 No exception here. 00:46 Common organisms include Cryptococcus neoformans, Coccidioides, Candida, Mucor. 00:55 Your focus, take a look, the letter C. 00:58 Letter C. 00:59 Cryptococcus, Coccidioides. 01:03 You could have Aspergillus, you could have Histoplasma, you could have blasto, they’re all here, right? But your focus will be on the first two, please. 01:12 Let’s talk about cryptococcal meningoencephalitis. 01:14 So I'm only going to focus upon a few here, the ones that are more common. 01:18 Most common, fungal infection of the CNS. 01:23 Typically, who’s your patient? Immunocompromised. 01:27 Do not confuse this with candida. 01:30 Well, how is the patient breathing in or should I say, what’s the access point? Maybe inhalation of spores from soil or maybe your pigeon crap. 01:42 In other words, your pigeon stool or excrement. 01:46 So think about all the different places where pigeons love to play. 01:50 Maybe you’re working in an office in which right outside your window, every morning, you are breathing in that lovely pigeon excrement. 01:58 Or maybe you are what, living underneath a bridge because you feel like camping out, I’m joking. 02:04 But a homeless person, underneath a tunnel or whatever, and then what happens? While, you sleep there, you might get pooped upon by a pigeon. 02:12 Anyhow, the point is, Cryptococcus. 02:15 “Protein headache.” Increased intracranial pressure. 02:21 And cranial nerve palsies are common presentations of cryptococcal. 02:25 It can have a very bland presentation, though. 02:27 Better keep that in mind. 02:29 So please look for your immunocompromised patient, most common fungal CNS infection, cryptococcal. 02:36 Let’s walk through in greater detail what you’re going to use. 02:40 To diagnose your patient with cryptococcal meningoencephalitis, in the CSF, you have lymphocytes. 02:46 Very low glucose and elevated protein. 02:49 I need you to keep this as being very important to you and you go back to that table and I grouped together viral and I put in fungal. 02:58 But here, make sure that you keep separate your Cryptococcus because this is the most common CNS infection. 03:06 India ink should come to mind immediately. 03:08 Cryptococcal antigen is highly sensitive and specific. 03:11 Make sure you know what Cryptococcus looks like, please, in microbiology. 03:16 Do that for me now. 03:19 Let’s continue. 03:20 Now, what’s interesting about chronic type of cryptococcal meningitis? Look where we are, the basal leptomeninges. 03:31 Why am I bringing this to your attention? Pay attention. 03:34 In the basal region, what if you were to then block the outflow of CSF from the foramen of Luschka or Magendie? Stop. 03:47 So now, you’re thinking about the lateral ventricles. 03:51 You know about your ependymal cells. 03:53 You’re producing CSF. 03:54 You go from your lateral ventricle, third ventricle, fourth ventricle, and then you should come out of your apertures to bathe the spinal cord, right? But what if you block that outflow? And you call this an obstructive, non-communicating type of hydrocephalus, interesting. 04:11 So if you’re confused about hydrocephalus, not to worry, we’ll talk about that in greater detail. 04:17 The antimicrobial therapy here, amphotericin B. 04:21 So let this be a good time for you to pay attention to some of your blood brain barrier type of pharmacology. 04:27 Here, we have amphotericin B. 04:29 We have others here as well, but for the most part, focus on amphotericin B.
About the Lecture
The lecture Fungal and Cryptococcus by Carlo Raj, MD is from the course CNS Infections - Clinical Neurology.
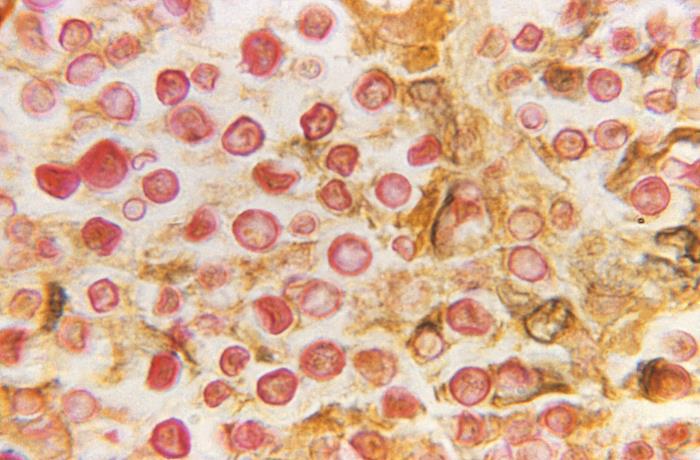
Included Quiz Questions
Which of the following patients are more susceptible to fungal meningoencephalitis?
- Patient with a history of recent kidney transplant
- Patient with a history of chronic hypertension
- Patient who works in a ship-building factory
- Patient with a history of chronic smoking
- Patient who is a microbiologist
A 20-year-old man who works in a bird shelter presents to the ER with a severe headache. His CD4 count is 200 cells/uL. He succumbs to meningitis after a few weeks. What is the most likely cause of his condition?
- Cryptococcus
- Histoplasma
- Aspergillus
- Candida
- Coccidiosis
A 45-year-old man with a history of HIV presents to your office with fatigue and headache for the last several days. His CSF shows lymphocytic pleocytosis and a positive India ink test. Which of the following is true regarding his condition?
- An obstructive noncommunicating type of hydrocephalus is a complication.
- A communicating type of hydrocephalus is a complication.
- Hydrocephalus is the least likely complication.
- Amphotericin B is not a drug of choice.
- Cryptococcal antigen is not sensitive.
Which of the following statements is true regarding the diagnosis of cryptococcal meningitis?
- The cryptococcal antigen test is highly sensitive and specific.
- The cryptococcal antigen test is neither sensitive nor specific.
- The cryptococcal antigen test is not specific but sensitive.
- The cryptococcal antigen test is not sensitive but specific.
- The India ink test is highly sensitive and specific.
Which of the following is not a drug of choice in the treatment of cryptococcal meningitis?
- Clotrimazole
- Amphotericin B
- Fluconazole
- Flucytosine
- Consolidation therapy
Author of lecture Fungal and Cryptococcus

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I love the combo of humour and medicine, it makes it sink in easily. Thanks once again Dr Raj for such a great lecture. I am just loving neuropathology with you, I hope I could be a guru like you :)
