Playlist
Show Playlist
Hide Playlist
Exertional Heatstroke: Symptoms & Management

-
Emergency Medicine Heat Illness.pdf
-
Download Lecture Overview
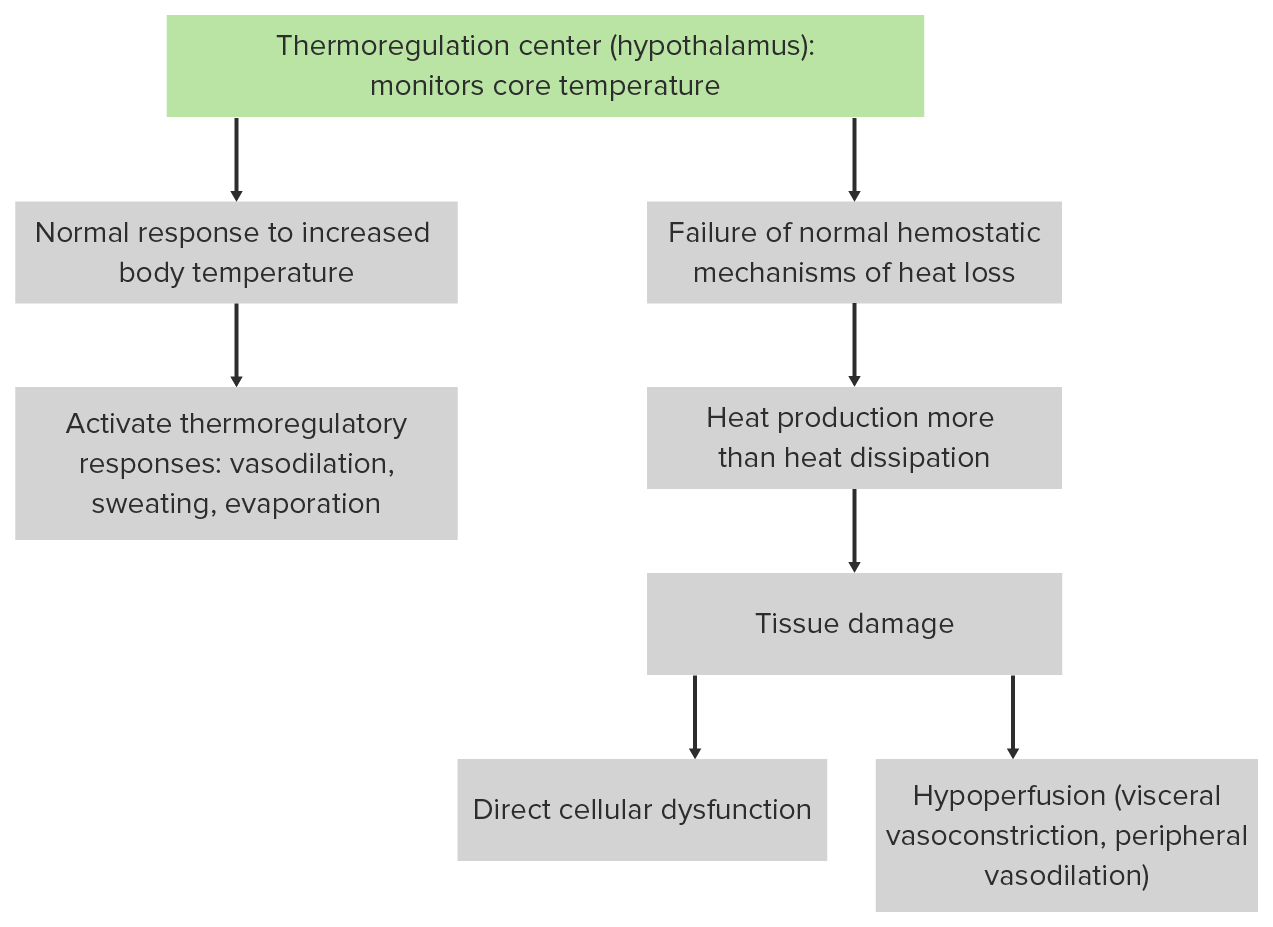
00:01 Alright, let’s move on to another case study. 00:03 So this time we have a 29-year-old man who’s running an Iron Man triathlon. 00:07 He collapsed during the last mile of it. 00:10 He’s a healthy guy, no past medical history. 00:13 It’s May but it’s an unseasonably hot day, so it’s 27 degrees out in the middle of May. 00:19 He comes in with the exact same vital signs as our last patient, so he’s got a significantly elevated core temperature, tachycardia, and tachypnea. 00:28 His skin is hot but he is diaphoretic. 00:31 His pupillary exam is normal. 00:33 His eyes are open. 00:35 He mumbles a little bit when you talk to him and he is able to localize pain. 00:39 So what’s the diagnosis for this gentleman? Is this another case of classic heatstroke? Actually not. 00:46 This is the other form of heatstroke which is exertional heatstroke and it’s physiologically a little bit different from classic, so we’re gonna talk about the differences between the two. 00:56 So typically, classic heatstroke affects elderly patients whereas exertional heatstroke is gonna affect young healthy people who are engaged in rigorous physical activity. 01:07 So classic heatstroke, you think patients who are debilitated. 01:10 Exertional, you think patients who are healthy. 01:13 Classically, you’re gonna see exertional heatstroke in the setting of athletic competition and training, but you also commonly see it in military recruits who are training vigorously in hot environments. 01:25 Classic heatstroke occurs pretty much only in the summer during heatwaves but exertional heatstroke can be sporadic. 01:32 So remember, skeletal muscle activity really significantly increases heat production and rigorous enough, exercise in pretty much any temperature setting has a potential of producing exertional heatstroke. 01:44 Of course, it’s much more common to see it when the patient is exercising in a hot environment. 01:50 Classic heatstroke patients are anhidrotic whereas exertional heatstroke patients will typically maintain the ability to sweat and will often present diaphoretic. 01:59 Typically, patients with classic heatstroke are gonna have a normal glucose level, whereas exertional heatstroke patients will have depleted their glycogen reserves and will often present hypoglycemic. 02:11 So it’s very, very important to check glucose in every patient with altered mental status and in those with exertional heatstroke, you might actually need to replete it. 02:19 Patients with classic heatstroke will almost never have lactic acidosis whereas those with exertional typically will. 02:27 Remember, these are patients who’ve been exercising very vigorously and they’ve often exceeded their anaerobic threshold in terms of their muscle metabolism. 02:37 So they’ve moved on to anaerobic metabolism and lactate production. 02:41 So they can come in with pretty severe lactic acidosis. 02:45 Exertional heatstroke patients often have much more significant liver damage as well and are much more likely than classic heatstroke patients to have severe coagulopathy or disseminated intervascular coagulation. 02:58 Classic heatstroke patients may present oliguric largely because of volume depletion whereas patients with exertional heatstroke will often come in with acute kidney injuries. 03:11 So they may have significant elevations in their creatinine often related to volume depletion and prerenal azotemia. 03:18 And then lastly, classic heatstroke patients typically don’t have rhabdomyolysis whereas exertional heatstroke patients very commonly do because again, they’ve been exercising so vigorously, they have significant muscle breakdown and leakage of muscle proteins into the vasculature. 03:36 So the management of exertional heatstroke is really the same as classic heatstroke. 03:42 There’s no difference between the two but you do need to recognize that these patients are more likely to have derangements of glucose and electrolytes, so they commonly are gonna need to have those things repleted and if they’re in rhabdomyolysis, they’re also gonna need to get aggressive IV fluid resuscitation and to maintain high volume urine output in order to prevent significant renal failure. 04:06 You also need to be aware that these patients are at higher risk for coagulopathy and DIC. 04:11 So you wanna make sure that you really keep close tabs on their coagulation status and correct any of those things if they come up abnormal. 04:20 So take home points on heat related illness. 04:24 It’s caused by a failure of normal heat homeostasis. 04:28 In the setting of heat stress, anytime you have a patient with a significantly elevated body temperature greater than 40 degrees and CNS dysfunction, you should definitely consider the diagnosis of heatstroke. 04:41 There are two different forms of heatstroke; classic and exertional, and you should know some important differences between the two. 04:47 However, they’re both treated with rapid cooling. 04:50 There’s a number of physiologic derangements that these patients can have and they’ll need supportive care for those and you should not treat them with antipyretics. 04:59 Thank you very much.
About the Lecture
The lecture Exertional Heatstroke: Symptoms & Management by Julianna Jung, MD, FACEP is from the course Toxicologic and Environmental Emergencies. It contains the following chapters:
- Exertional Heatstroke
- Symptoms of an Exertional Heatstroke
- Management of an Exertional Heatstroke
Included Quiz Questions
Which of the following statements regarding classic and exertional heatstroke is NOT true?
- Both cases will present with anhidrosis
- Exertional heatstroke is most commonly seen in younger patients
- Lactic acidosis can be observed in exertional heatstroke
- Both may cause renal injury
- Rhabdomyolysis may be observed in patients with exertional heatstroke
What is the mainstay of treatment for exertional heatstroke?
- Rapid cooling
- Antipyretics
- Glucose repletion
- Vasopressors
- Anticoagulation
Author of lecture Exertional Heatstroke: Symptoms & Management

Julianna Jung, MD, FACEP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Phenomenal teacher, really. You are a gem, ma'am - big fan!
