Playlist
Show Playlist
Hide Playlist
Encephalitis: Diagnosis



-
Slides Encephalitis InfectiousDiseases.pdf
-
Reference List Infectious Diseases.pdf
-
Download Lecture Overview
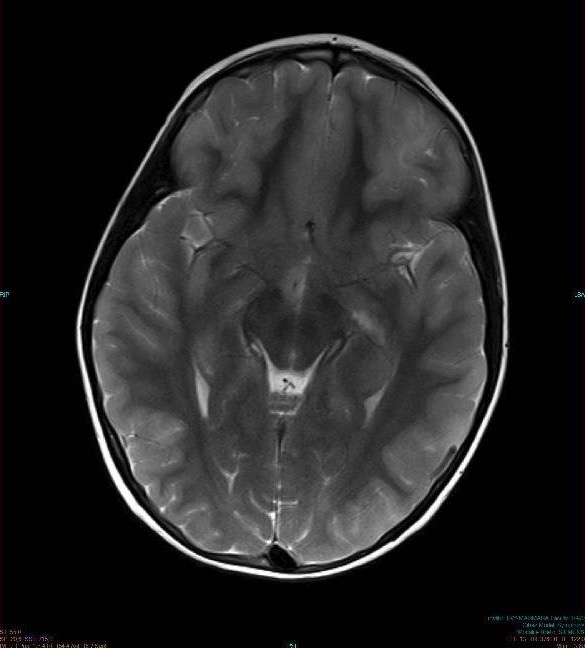
00:02 Now, when somebody comes in with altered mental status and signs of encephalitis, we certainly are going to examine the cerebrospinal fluid if it's safe. 00:13 And so, what we’re going to look for is the cytology. 00:16 And what you would expect, unlike bacterial meningitis, is a lymphocytic pleocytosis. 00:24 There may be some neutrophils there, but there is a predominance of mononuclear cells. 00:30 Unlike bacterial meningitis, your glucose is normally not low. 00:38 The protein may be elevated. 00:42 Those are the classic findings, but the exceptions to the rule are the West Nile virus, which may have more neutrophils in it and Eastern equine encephalitis may have a neutrophil predominance. 00:57 And the cell count is going to be 50 to 500 cells. 01:03 To make a specific diagnosis, we have to rely on PCR and antibody studies. 01:10 The herpes simplex PCR is very sensitive and very specific and we use it all the time. 01:19 For varicella zoster, it's not nearly so sensitive, but it does have a high specificity. 01:25 Culturing these viruses is not particularly useful. 01:32 So, serology is important and we’re going to get an acute serum on admission and then periodically get convalescence serum, looking for antibody rises. 01:46 We can do PCR on gastrointestinal samples, respiratory secretions and skin vesicles and they're pretty sensitive and specific. 01:55 But if we just can't figure out why the patient has encephalitis and the patient is deteriorating, then we may need to resort to a brain biopsy. 02:07 These are usually done through a burr hole and a needle aspirate. 02:17 Neuroimaging is important in patients who have encephalitis and the MRI is the study of choice. 02:24 And particularly, in herpes simplex virus, 90% of the time you're going to be looking in the temporal lobes. 02:34 Varicella zoster produces multifocal hemorrhage and infarction and a West Nile virus has less frequent abnormalities than herpes simplex virus. 02:50 We don't do EEG very often, but if you were to do it, you'd find generalized slowing in most forms of encephalitis. 02:59 And in herpes, you’d find, once again, abnormalities like spikes in the temporal lobe. 03:07 And you’d find that in a majority of patients with herpes virus encephalitis. 03:14 And this, for example, is what herpes virus encephalitis looks like. 03:19 Notice the predominance in both temporal lobes in this patient. 03:25 Notice the multifocal location in the patient with varicella zoster encephalitis. 03:32 And notice that in West Nile virus, the encephalitis is highlighted by increased signal in the basal ganglia. 03:41 And remember, we talked about parkinsonism, and so that fits with West Nile virus. 03:50 The enteroviral encephalitis, you can have increased signal in both hemispheres.
About the Lecture
The lecture Encephalitis: Diagnosis by John Fisher, MD is from the course CNS Infection—Infectious Diseases.
Included Quiz Questions
Which of the following abnormalities would you CLASSICALLY expect to see on cerebrospinal fluid cytology studies in the case of viral encephalitis?
- Lymphocytic pleocytosis
- Elevated glucose
- Decreased glucose
- Decreased protein
- Neutrophil pleocytosis
Which of the following encephalitic viruses is most likely to present with neutrophilic pleocytosis early during the course of infection?
- West Nile virus
- Herpes simplex virus
- Varicella zoster virus
- Western equine encephalitis virus
- Japanese encephalitis virus
Which of the following describes the sensitivity and specificity of herpes simplex virus (HSV) polymerase chain reaction (PCR)?
- High sensitivity, high specificity
- Low sensitivity, low specificity
- Low sensitivity, high specificity
- High sensitivity, low specificity
Bilateral asymmetrical involvement of the limbic system on MRI, including the medial temporal lobes, insular cortices and inferolateral frontal lobes, and cingulate gyri, is typically seen in infection with which of the following types of pathogens?
- Herpes simplex virus
- West Nile virus
- Varicella zoster virus
- Western equine encephalitis virus
- Japanese encephalitis virus
Which of the following electroencephalogram (EEG) patterns is most characteristic of herpes simplex virus encephalitis?
- Nonrhythmic temporal and frontotemporal slowing
- No abnormalities are typically seen on EEG
- Polymorphic delta activity in the motor cortex
- Increased brain activity localized to the cerebellum
- Generalized intermittent rhythmic delta slowing
Author of lecture Encephalitis: Diagnosis

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
