Playlist
Show Playlist
Hide Playlist
Dissection of the Aorta: Therapy

-
Slides 05 VascularMedicine advanced.pdf
-
Reference List Vascular Medicine.pdf
-
Download Lecture Overview
00:01 Now, let's talk a little bit about therapy of dissecting aortic aneurysms. The medical therapy consists of controlling hypertension, since the high blood pressure is really putting a lot of stress on the aneurysm. You want to decrease the force of systole, and this is done, in an emergency with dissection, with intravenous drugs. Intravenous sodium nitroprusside and beta-blocking drugs markedly decrease the pressure, and they decrease the stress on the aneurysm. Since dissections can be fatal because of rupture, usually there is some form of intervention—either surgery or angioplasty with a stent to control the aneurysm. In the picture shown here (this is a surgical picture), this is actually a dilated aneurysm, not a dissecting aneurysm, but the operation is the same. You resect the aneurysmal area, and you put in a graft—usually a Dacron prosthetic graft to replace the diseased segment of the aorta. 01:05 When it's in the chest, as this is, it's a very big operation. It's a big operation in the abdomen too, and these days, there's a strong movement to do as many of these as possible with catheters and stents rather than making a major surgical intervention. 01:25 Just to remind you that although dissection is a life-threatening condition, they are much less common compared to the abdominal aortic aneurysm. This is really… And it's shown here, in a slide, a pathology specimen shows you a clotted abdominal aortic aneurysm. 01:45 This is much more common than dissection, and usually, the symptoms are much less impressive. 01:50 The dissection patient has severe, maximum symptoms at the onset. The chronic dilated aneurysms may cause intermittent, sort of nagging pain, but usually (unless they rupture) won't cause the severe pain that the dissection causes.
About the Lecture
The lecture Dissection of the Aorta: Therapy by Joseph Alpert, MD is from the course Arterial Diseases.
Included Quiz Questions
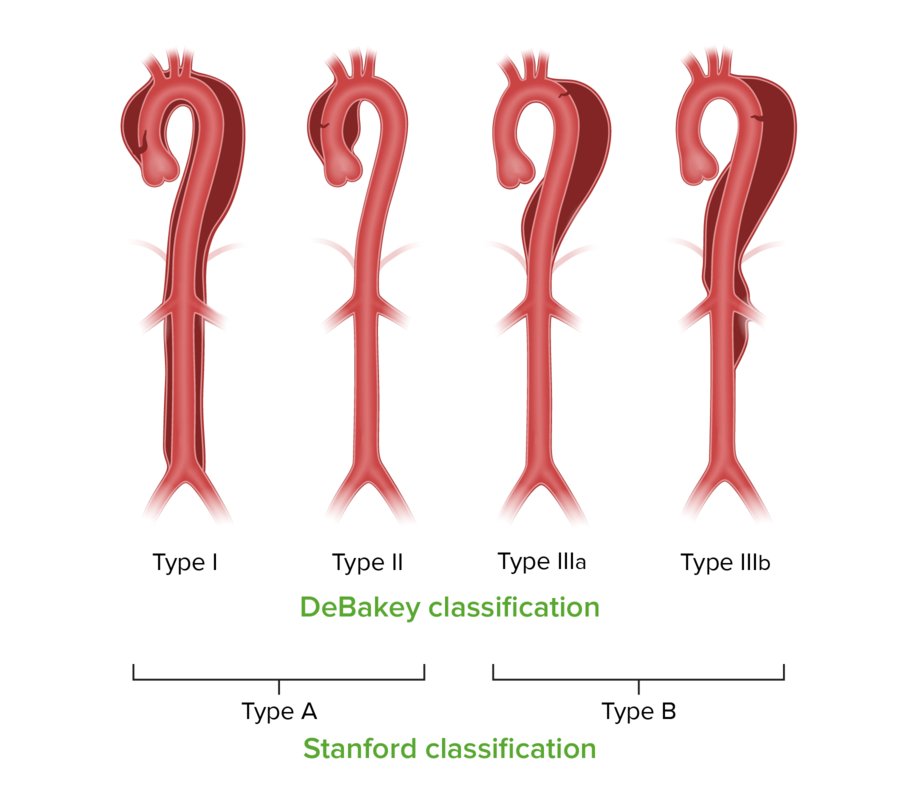
A DeBakey type 1 (Stanford type A) dissection of the aorta involves which of the following:
- The ascending aorta.
- The descending aorta.
- The brachial artery.
- The celiac artery.
Author of lecture Dissection of the Aorta: Therapy

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
