Playlist
Show Playlist
Hide Playlist
Diaphragmatic Hernia and Congenital Cystic Adenomatoid Malformation (CCAM)

-
Slides Pulmonary Disease Newborns.pdf
-
Download Lecture Overview
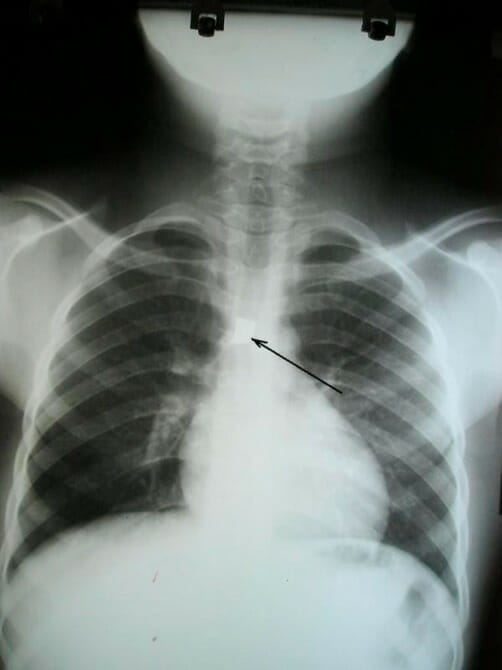
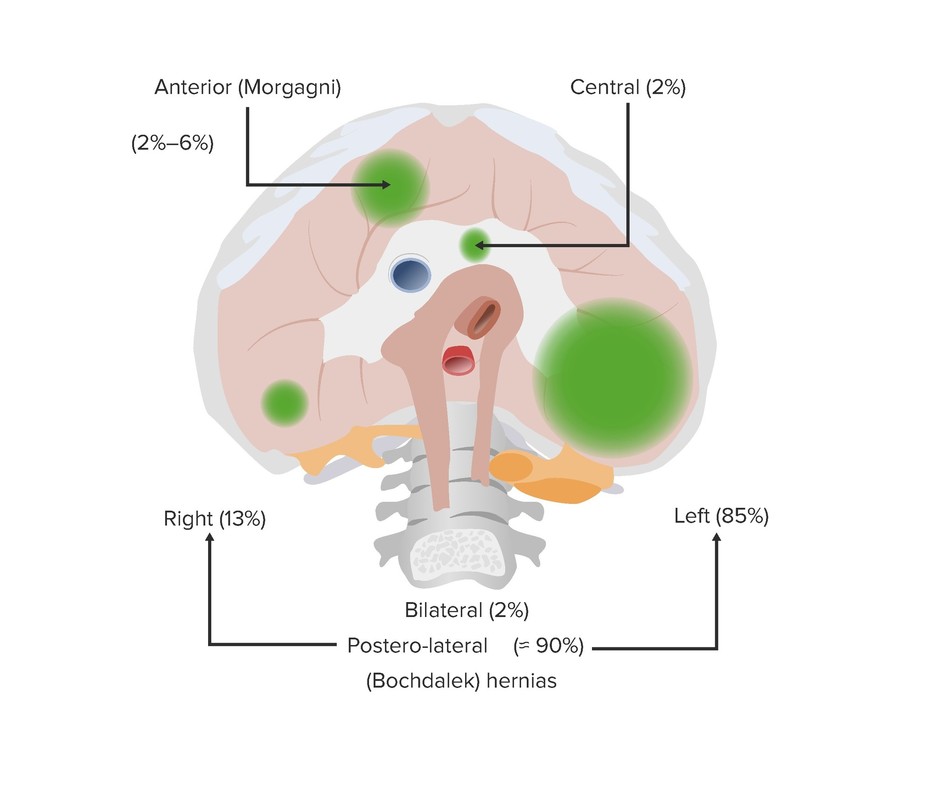
00:01 Let’s switch gears now to diaphragmatic hernia. 00:04 This is a really unique problem in newborns, which is very challenging to manage. 00:11 So in this situation, a baby is born where the intestines have worked their way through the diaphragm and up into the chest. 00:22 So, other things may go through so it might not just be the intestines, it might as well be the stomach, the patient may have some liver up in the chest, or the spleen may even get into the chest. 00:35 But in most cases it’s the intestines that have migrated up into the chest. 00:41 There are several different types of congenital diaphragmatic hernia and the names of them are sometimes found on various tests. 00:51 So, the Bochdalek is about 90% of congenital diaphragmatic hernias and it’s much more common on the left side, as is pictured here in this x-ray, than on the right side. 01:06 Generally, this is a posterior lateral, in the back of the diaphragm hole, where the intestines are squirting up into the thoracic cavity. 01:19 This is preventing the lungs from developing appropriately and these children will have respiratory distress at birth. 01:28 The Morgagni is another type, which is much rarer, and this is more in the front, anterior, and just behind the sternum. 01:37 And this is about 2% to 6% of cases. 01:40 This is another type of hernia. 01:43 Lastly, rarely, patients can have a very bad hiatal hernia, where at the entrance of the esophagus down to the diaphragm, it’s simply wide open in the stomach and other intestinal contents can make their way into the thoracic cavity. 01:59 In these patients, it’s surprising, but the diagnosis may be tricky and delayed. 02:06 These patients will often present with intestinal sounds heard in the chest. 02:14 So, that intestinal rumbling, the borborygmi, if that’s heard in the chest, a chest x-ray is absolutely indicated. 02:24 Occasionally, this can be diagnosed much later in life. 02:29 I have a colleague who was diagnosed at the age of 40. 02:34 Patients may have a scaphoid abdomen, where it’s sucked in, and you can see that ridge of the lower ribs as that abdomen is sucked in because the intestinal contents have come up. 02:45 And they may have associated genetic syndromes. 02:50 Diaphragmatic hernias are more common in some of the trisomy patients, specifically Down syndrome or trisomy 21, or Patau syndrome or trisomy 13. 03:03 In the diaphragmatic hernia patient, if it’s known, these patients will generally be intubated at birth and they will provide positive pressure through an ET tube to try and help those lungs stay open. 03:16 In severe cases, they may have to do ECMO or extracorporeal oxygenation of the blood through a machine that bypasses the heart and lung entirely. 03:28 We do want to evaluate these patients for pulmonary hypertension because since they have less pulmonary structure, they may have increased pressures on the right side. 03:38 And when these patients are stable, we will undergo a surgical repair to try and fix the problem and get the intestinal contents back down below the diaphragm. 03:50 Lastly, let’s switch to congenital cystic adenomatous malformations or CCAMs for short. 03:57 The CCAM are cysts that are found within lung parenchyma and you can see one pictured here on this CAT scan. 04:04 These things may be single or they may be multiple and these cavernous malformations prevent the adequate growth of normal lung tissue. 04:15 They can lead to air trapping and they may harbor infections or become abscesses. 04:22 They may grow slowly. 04:24 It’s not uncommon for one to be reasonably small and then gradually continue growing through life and require resection. 04:31 They also do have some malignant potential so these are generally excised. 04:37 And usually, we like to surgically remove them before one year of age. 04:44 That’s a good summary of most of the important congenital or around birth respiratory conditions in children. 04:52 Thanks for your attention.
About the Lecture
The lecture Diaphragmatic Hernia and Congenital Cystic Adenomatoid Malformation (CCAM) by Brian Alverson, MD is from the course Pediatric Pulmonology.
Included Quiz Questions
What is the most common type of congenital diaphragmatic hernia?
- Bochdalek
- Morgagni
- Hiatal
- Ventral
- Indirect
Which of the following statements is TRUE regarding congenital diaphragmatic hernia?
- Respiratory distress may be delayed or absent.
- Intestinal sounds are heard in the groin.
- They usually have protuberant abdomen.
- They are never associated with any congenital syndromes.
- The diagnosis is obvious at the time of birth in all cases.
All of the following statements are true regarding Congenital Cystic Adenomatoid Malformation (CCAM), EXCEPT?
- Only a single lesion will be found.
- Cysts are found within the lung parenchyma.
- It may lead to air trapping and may harbor infection.
- It may grow slowly or become malignant.
- Should be removed surgically before one year of age.
Author of lecture Diaphragmatic Hernia and Congenital Cystic Adenomatoid Malformation (CCAM)

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Important topic for neonatal medicine. All the information to suspect the disease is contained within the lecture. Thank you!
