Playlist
Show Playlist
Hide Playlist
Diagnosis of Acute PE

-
Slides 08 VascularDiseases RespiratoryAdvanced.pdf
-
Download Lecture Overview
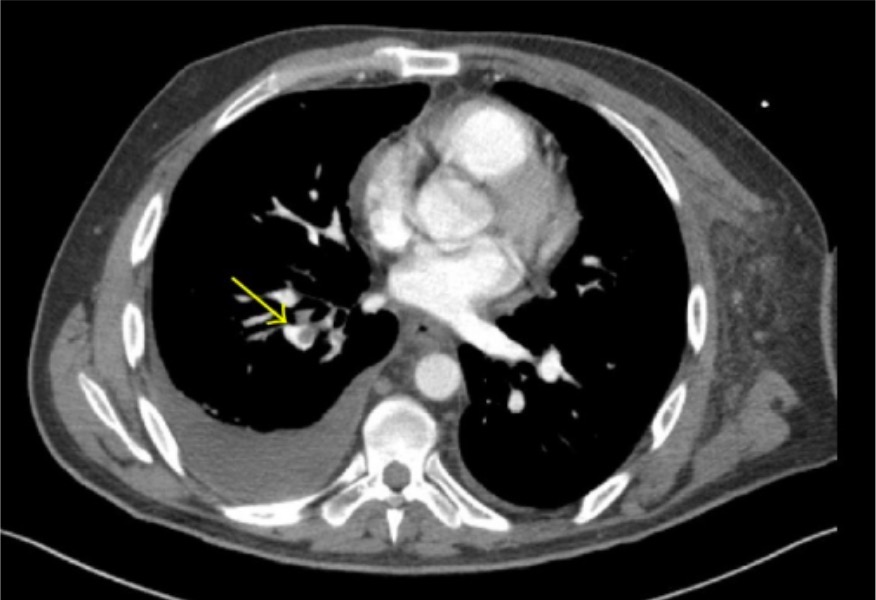
00:01 To make a diagnosis, well if you can show that there is new, right ventricular strain, then that would suggest there has been a large PE, and to do that an echocardiogram is very helpful. It's a bedside test, it's very quick and it can show the very significant right ventricular strain that you get with very large PEs in a very short period of time. 00:23 In addition, you may have the raised brain natriuretic peptide levels suggestive of cardiac problems, and there might be a raised troponin T and the ECG can show signs of right ventricular strain, inverted T waves V1 through to V3 and then there's the specific ECG findings you often get in, what can get in pulmonary emboli of a S wave in lead 1, a Q wave in lead 3, with T-wave inversion in lead 3 which is the classical ECG abnormalities you see in somebody presenting with acute PE which is present in a minority of patients unfortunately. 00:58 CT scan is now the main way for identifying PEs, and this is a specific type of CT scan called CT pulmonary angiography, where you inject contrast into the vein and that will flow to the heart, and then be sent down the pulmonary arteries and that allows you to see the clots as filling defects in the pulmonary arteries as shown by this example here; the arrows are pointing to central pulmonary arteries, and you can see they are partly grey which represents the clot and the white is the contrast which is finding it difficult, but just going around the outside of that clot. And this is a standard test now for identifying the presence of pulmonary emboli. In the past, and for some patients we still use a radioisotope scan called ventilation perfusion scan, where you're looking for mismatched defects in perfusion, that means that the patient is ventilating that part of the lung, so the radioisotope which is inhaled is seen in that area, but the perfusion of that part of the lung, the radioisotope that reaches that part through the pulmonary artery is reduced, so it's a mismatched defect that occurs in a VQ scan. That's less commonly used nowadays because of the greater rapidity and ease of getting CT scans. 02:21 The chest X ray itself actually is very nonspecific, it sometimes shows reduced vascular markings but is a very poor test to identify somebody who may have a pulmonary clot. Occasionally we need invasive pulmonary angiography, but that's only rarely needed. 02:37 You can also, using the radiology, see evidence of the lung damage that's been caused by the clot and this is the infarcts that I was talking about earlier, where the tissue distal to where the clot is occurred has been damaged and has infarcted and causes a focal area of consolidation which classically would be a wedge-shaped pattern based on the pleura. 02:58 And this is CT scan here, and you can see the clot in the proximal part of the artery and then distal to that is the patch of grey, which represents the damaged tissue of the lung due to infarction. 03:10 If you suspect somebody has a PE, another way of making the diagnosis or at least making the decision about whether they require treatment for the pulmonary embolus is to look for a deep vein thrombosis, and this is very easy using a noninvasive ultrasound Doppler test of the leg. And if you identify somebody that has a DVT, the treatment of that is the same as it is for a PE, so that's adequate in many circumstances to give you the information that you need to start patients on treatment. In addition, we do blood tests occasionally to look for evidence of coagulopathy, for example the blood D dimer level is usually raised when patients have pulmonary emboli or DVTs, however it's a nonspecific blood test, and is often raised for many inflammatory conditions and therefore, isn't terribly helpful in identifying a patient who may have a PE versus a pneumonia or other differential diagnosis. 03:58 If somebody has recurrent pulmonary emboli or DVTs or a family history of pulmonary emboli, then we often do blood tests to look for inherited disorders of coagulation such as protein CNS deficiencies, which may make them more likely to have PEs, and these patients often need a lifelong anticoagulation to prevent further PEs occurring.
About the Lecture
The lecture Diagnosis of Acute PE by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Pulmonary Vascular Disease.
Included Quiz Questions
A 54-year-old woman has sudden onset of dyspnea with tachycardia and hypotension 3 days after a hysterectomy. Which of the following would be a nonspecific finding to support a diagnosis of a pulmonary embolus?
- Raised serum D-dimer level
- A positive V/Q scan
- Right ventricular strain on echocardiography
- A large filling defect in the right pulmonary artery visible on CT pulmonary angiogram in the right pulmonary artery
- ECG showing Deep S wave in lead 1 and inverted T wave in lead 3
Which of the following is the ECG abnormality commonly observed in pulmonary embolism?
- A deep S wave in lead 1, a deep Q wave in lead 3, and an inverted T wave in lead 3
- Peaked T waves, short QT intervals
- Widened QRS complex
- Presence of U waves
- Missed P waves
Which of the following is the imaging modality of choice to look for evidence of deep vein thrombosis (DVT)?
- Doppler ultrasound
- CT scan
- MRI scan
- Chest X-ray
- Angiography
Author of lecture Diagnosis of Acute PE

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
