Playlist
Show Playlist
Hide Playlist
Development of the Subcardinal Anastomosis

-
Slides 06-33 Cardinal Veins and the Large Veins.pdf
-
Reference List Embryology.pdf
-
Download Lecture Overview
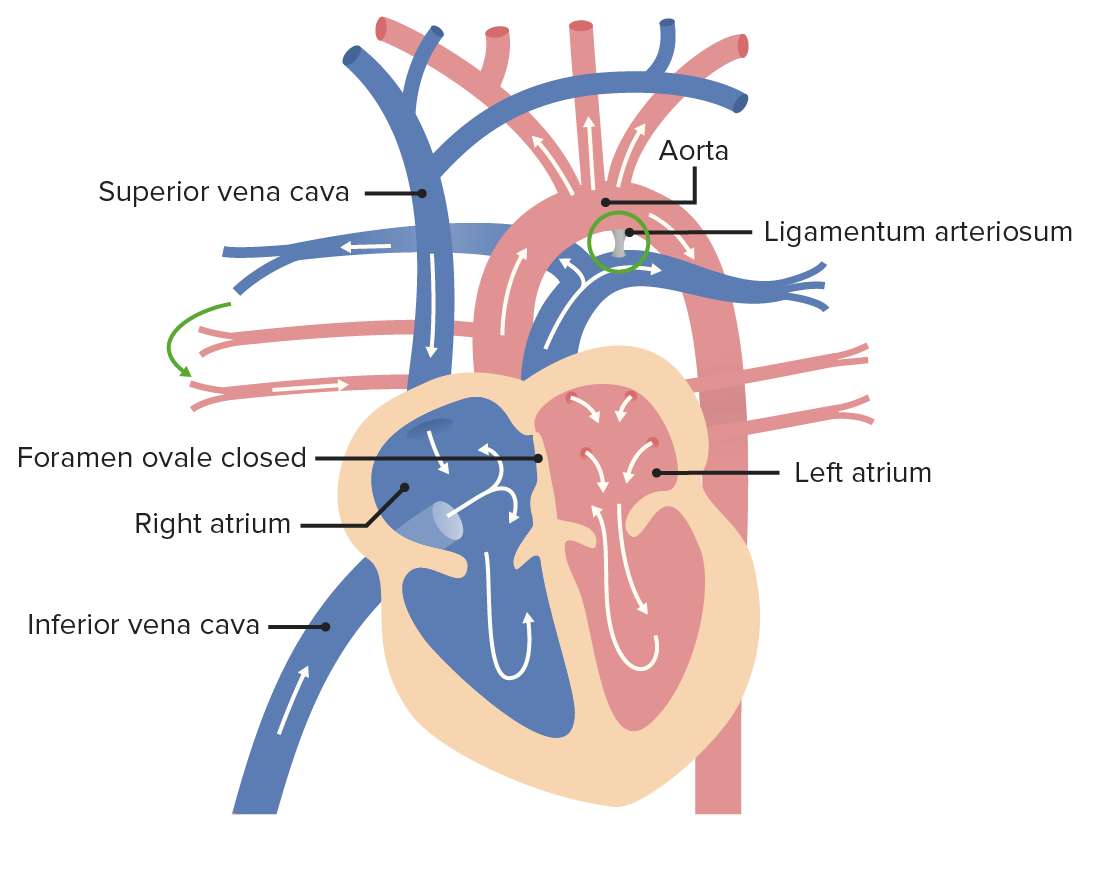
00:01 Now, let's move on and discuss how the common cardinal veins and it's various tributaries make the large vessels of the body wall, like the superior and inferior vena cava. 00:12 Essentially, we have a common cardinal vein bringing blood to the heart and on both the right and the left, we have anterior cardinal veins going towards the head and posterior cardinal veins going towards the developing feet. 00:25 The posterior cardinal veins develop a group of veins growing forward ventrally from them called the subcardinal veins, and they're actually gonna grow so far anteriorly that they meet up at the subcardinal anastomosis. 00:40 So, in blue, stretching down the body we have posterior cardinal veins and in red we have the subcardinal anastomosis. 00:49 At the same time, blood from the lower limbs is leaving them through the iliac vein and going into the posterior cardinal veins to get back to the heart. 00:59 Likewise, in the upper limb, we're going to have subclavian veins bringing blood back to the heart as well and we'll track the formation of the mature subclavian and iliac veins as we proceed. 01:11 That subcardinal anastomosis gets more and more sophisticated and at the same time the body decides it wants another set of veins coming off the posterior cardinal veins. 01:21 These are called the supracardinal veins. 01:24 And they're gonna be extending posteriorly off the posterior cardinal veins and heading down towards the legs. 01:30 And what's interesting about them is they are largely going to displace and replace the posterior cardinal veins that they originate from. 01:37 So they're gonna stretch posteriorly, the subcardinal anastomosis are stretching anteriorly and the posterior cardinal veins are going to really kinda meet up with the iliac veins in both the right and left and start draining blood from the lower limb. 01:53 What's going to be very interesting is as more blood travels through the supracardinal venous system, less blood is travelling to the posterior cardinal veins and less blood equals less pressure, less pressure means those arteries'not arteries, pardon me, veins, are gonna get smaller and smaller, and eventually rescind. 02:13 Now, the inferior vena cava had started to come into existence. 02:18 We had the vitelline veins, going through the liver. 02:21 They've connected to the subcardinal anastomosis, so our earliest little view of the inferior vena cava comes into existence now. 02:30 It's connecting to the subcardinal anastomosis and the subcardinal anastomosis is gonna start draining the organs that are developing more posteriorly. 02:38 So we know that the gut tube is gonna be drained by the hepatic portal veins, which are coming from the vitelline, but kidneys and other developing structures like the gonads that are more posterior, are gonna be drained by the subcardinal anastomosis. 02:52 I wanna jump up towards the head and upper limb for a second and note that the anterior cardinal veins are now receiving blood from the head, the neck, and the upper limb. 03:04 So the jugular and subclavian veins are coming into existence up there draining to the common cardinal vein and then to the heart. 03:12 At this time, circulation and venous return is more or less symmetric on both sides. 03:18 But that symmetry is about to breakdown. 03:21 And it breaks down because anastomosis or connections start to form between the right and left iliac veins and the right and left anterior cardinal veins. 03:34 That's gonna be called the iliac anastomosis in the lower limb, and the left and right brachiocephalic anastomosis in the upper limb. 03:43 So that brachiocephalic anastomosis connects our jugular vein on the left, jugular vein on the right. 03:50 Subclavian vein on the left, subclavian vein on the right, and brings them together and then blood will travel to the common cardinal veins and the heart. 03:58 As this is happening in the lower portion of the body, we're going to have the poster cardinal veins almost entirely disappear. 04:07 The remaining connected to the common cardinal vein, the remaining connected down in the area of the iliac anastomosis but in yellow, the supracardinal veins have largely displaced them and are receiving blood on the right and left from the iliac veins travelling up to the common cardinal veins and then to the heart. 04:28 Meanwhile, the subcardinal anastomosis is not only draining blood from the kidneys and the developing gonads, it's developed additional connections to the supracardial anastomosis. 04:41 So the veins on the front and back of the developing body wall are now interconnected and connected to the blood drainage from the lower limb and the upper limb. 04:52 And finally, what's going to happen is on the left side, we're gonna lose the connection between the iliac vein and the supracardinal vein and thereafter, all the blood from the lower body, both iliac veins is gonna drain to the supracardinal vein on the right and it's going to enlarge. 05:10 It will then travel into a derivative of the subcardinal anastomosis and then to the vitelline portion of the inferior vena cava. 05:19 So the inferior vena cava has come into existence and it's coming from, get this, the iliac veins, a small portion of the posterior cardinal vein, a portion of the right supracardinal vein, the subcardinal anastomosis, and finally, the vitelline vein. 05:37 That's a lot going on to make that one large vessel that's on the right side of our body. 05:43 So after all of these, you'll note, that the posterior cardinal vein have largely disappeared the only remnant of them is very close to the common cardinal veins up near the point where it drains into the heart. 05:55 But at the same time, the supracardinal veins on the left and right are still there and still hanging out in the posterior portion of the body wall. 06:03 They're gonna develop an anastomosis between the right and left side as well. 06:08 So one of the major features of venous drainage and development is that we're gonna have anastomoses from right to left develop and in this case, the supracardinal veins are gonna be left as what you call the azygos veins. 06:22 On the right, we have the azygos vein draining up to a remnant of the posterior cardinal vein and then into the superior vena cava. 06:28 And then on the left, we have the hemiazygos and accessory hemiazygos veins that connect to the azygos veins and all the way up again to the superior vena cava. 06:38 These are all remnants of the supracardinal veins that came into early existence and replaced the posterior cardinal veins. 06:48 If we turn our attention to the upper limb and blood drainage of the head, we can note that the jugular veins are bringing blood in to the anterior cardinal vein system. 06:58 The subclavian veins are bringing blood into that system and the right and left side are connected by that brachiocephalic anastomosis. 07:05 At this point, blood could either drain down the right to the superior vena cave, or to the left, which is going to become the coronary sinus of the heart. 07:13 So we have two potential pathways for venous blood to return to the heart. 07:17 But that's not how things are going to stay. 07:19 In the adult, we have all of the blood from the upper limb and head and neck drain to the right side and the superior vena cava and that's because the coronary sinus is the only remnant of the left side of that anterior cardinal vein. 07:35 Essentially, it's going to detach from the rest of the venous system and where it was partially draining the left side of the body before, the coronary sinus only drains the heart once development is complete. 07:47 Now if we look at this slide, we can see how the mature large vascular structure has come into existence from all this complicated and all these veins have come together and replaced one another and the process has proceeded. 08:02 So what can go wrong? That's actually a really good question because venous variation is incredibly common. 08:09 Veins can take a variety of pathways to get where they need to go and as long as the blood gets back to the heart, it doesn't cause any real clinical problems. 08:18 And many people are walking around with massively interesting venous malformations that have no clinically important signs. 08:26 One thing that can happen is if you have failure of the anastomosis on the right and left to connect, you can wind up with some odd blood drainage patterns. 08:34 If the brachiocephalic anastomosis between the right and left anterior cardinal veins doesn't develop, you can wind up with your right side blood drainage going to the superior vena cava and your left side, blood drainage from the head and upper limb, going into the coronary sinus of the heart and then draining into the right atrium there. 08:54 This may not be something that's clinically evident because the blood does get where it belongs. 09:00 It gets to the right atrium even though it's taking a very odd path to get there. 09:04 Another thing that can happen is you can have a connection between the posterior cardinal vein and the supracardinal vein, persists on the left side and typically we have our inferior vena cava, pretty much only on the right side. 09:17 But if you had that persistent artery you then have a persistent left inferior vena cava or double inferior vena cava draining blood from the lower limbs up to the heart and also through the renal system to the rest of the inferior vena cava. 09:33 Once again, these can be experienced only when you're doing imaging studies or in surgery for the first time because they don't cause clinical problems in and of themselves, but they can create problems in surgery if they are not accounted for. 09:46 Now, something that is clinically important and potentially fatal is total anomalous pulmonary return. 09:53 One thing we didn't draw a lot of attention to was that the pulmonary veins are draining to the left side of the developing atrium, and as the right and left atria separates, we wind up with the pulmonary veins draining to the left atrium and the superior and inferior vena cava draining to the right atrium. 10:11 Occasionally, the pulmonary veins can attach too far to the right, and wind up draining to the wrong set of vessels. 10:19 And these total anomalous pulmonary return, basically means that the oxygenated blood from our lungs can go to the wrong place and instead of being pumped around our body, it can mix with blood from somewhere else. 10:32 Now, most commonly, it can wind up draining to the right atrium but I can also go to any of the nearby large veins, like the superior vena cava, the inferior vena cava. 10:41 They can drain into the brachiocephalic anastomosis or which gonna become the left brachiocephalic vein and the major problem is that you've got your arterial blood mixing with venous blood before it's gonna have a chance to get to anywhere in the body causing a massive right to left shunt and very probable cyanosis, if the blood is then able to permeate the rest of the body. 11:04 You're gonna need to have some sort of an atrial or ventricular septal defect to allow this blood to get in to the aorta in the first place. 11:11 So that is TAPVR, total anomalous pulmonary return. 11:16 It’s hypothesized that this anomaly results from impaired expression of the cardiac-specific atrial natriuretic factor promotor, which is usually repressed in patients. This is most likely due to a de novo mutation in A N K R D 1 gene. 11:35 Thank you very much for your attention, and I'll see you in our next talk.
About the Lecture
The lecture Development of the Subcardinal Anastomosis by Peter Ward, PhD is from the course Development of Thoracic Region and Vasculature. It contains the following chapters:
- Development of the Subcardinal Anastomosis
- Malformations of the Veins
Included Quiz Questions
What vein that drains into the posterior cardinal veins forms a venous network in the developing kidney?
- Subcardinal vein
- Supracardinal vein
- Common cardinal vein
- Iliac vein
- Renal vein
What vein that develops off of the posterior cardinal vein drains the posterior aspect of the body?
- Supracardinal vein
- Subcardinal vein
- Common cardinal vein
- Iliac vein
- Renal vein
The inferior vena cava begins to form as the right vitelline vein fuses to what other structure?
- Subcardinal anastomosis
- Subcardinal vein
- Supracardinal vein
- Posterior cardinal vein
- Common cardinal vein
Which of the following veins do not drain into the inferior vena cava?
- Azygos vein
- Right vitelline vein
- Subcardinal anastomosis
- Right supracardinal vein
- Right posterior cardinal vein
The coronary sinus is the remnant of what embryonic vessel?
- Left common cardinal vein
- Right common cardinal vein
- Anterior cardinal vein
- Posterior cardinal vein
- Azygos vein
Which of the following statements regarding the malformation of veins is FALSE?
- Venous malformations are almost always symptomatic and more severe than arterial malformations.
- Failure of the development of the brachiocephalic anastomosis causes the blood from the left subclavian and jugular veins to drain into the coronary sinus and then to the right atrium.
- A double inferior vena cava forms between the left common iliac and left renal veins if the connection between the left posterior and supracardinal veins remains.
- The total anomalous pulmonary venous return occurs when the pulmonary vein enters the right side of the primitive atrium or sinus venosus.
- Total anomalous pulmonary venous return is fatal unless another right to left shunt malformation is simultaneously present.
Author of lecture Development of the Subcardinal Anastomosis

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
