Playlist
Show Playlist
Hide Playlist
Cryptorchidism

-
Slides Introduction Male Repro.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
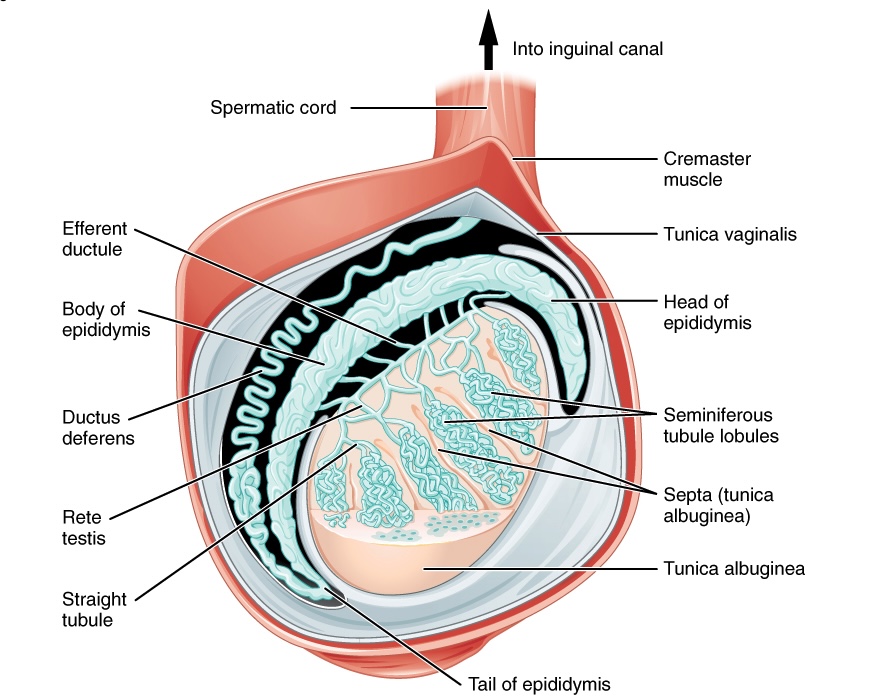
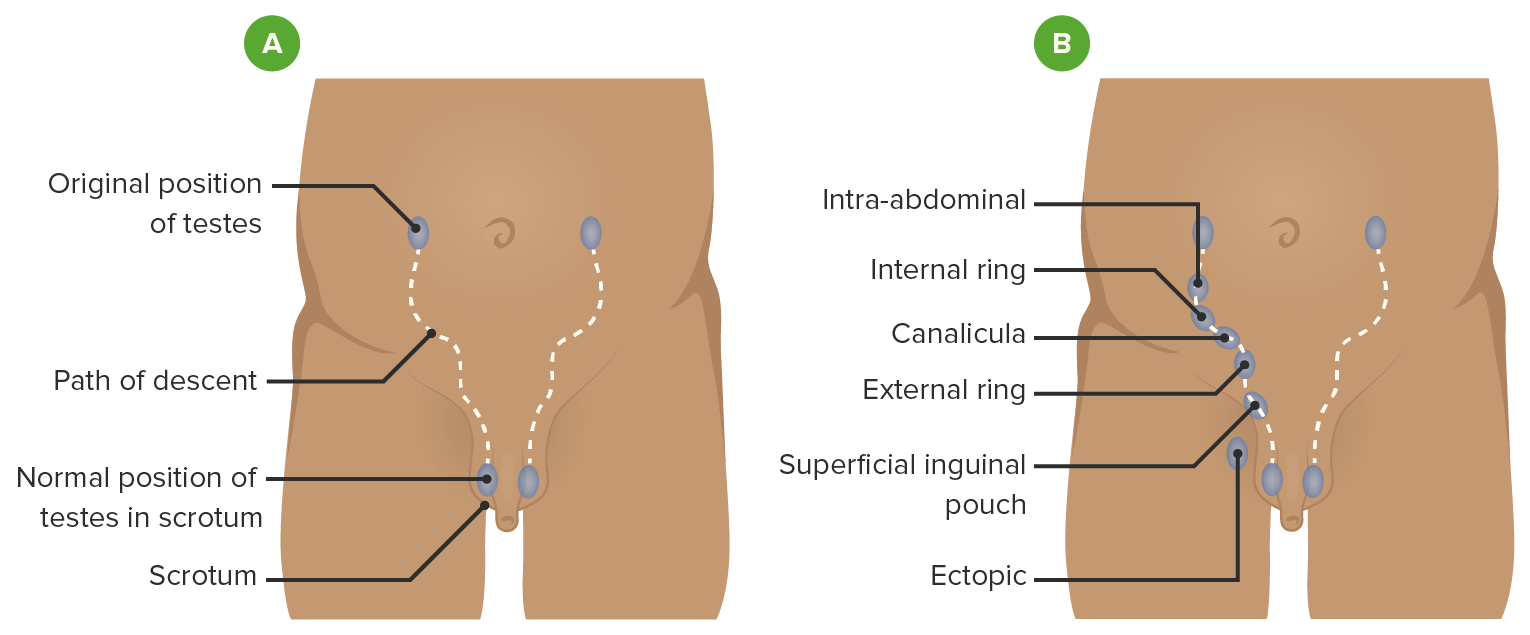
00:00 In this section, we’ll take a look at the remainder of our male reproductive tract. 00:07 We have completed our discussion of penile pathology here. 00:10 We’ll take a look at pathology of testis, epididymis, and the scrotum. 00:14 Once again, picture what these look like. 00:17 know as to where we are, so that you’re able to clearly understand the pathogenesis of each one of these conditions. 00:25 Our topic at first is cryptorchidism. 00:28 When I began the discussion, we began our male reproductive by looking at congenital issues embryologically. 00:35 And we looked at the testis beginning in the abdomen and if it’s not properly pulled down by the gubernaculum into the scrotum, this is then called cryptorchidism. 00:45 Let’s go into details. 00:46 One or both undescended testis. 00:49 Majority of which are located in the inguinal canal. 00:52 Can you picture that? Normally, they should be resting in the scrotum. 00:56 However, it didn’t quite make it and the testis is stuck in the inguinal canal Majority of them are. 01:03 Could they be back in the abdomen? Sure. 01:05 But go with the common. 01:07 There’s impaired spermatogenesis, as you can imagine, if the testis aren’t properly located in the scrotum. 01:12 You need that optimum temperature of 37 degrees, right? And if you don’t have that 37 degrees Celsius, then it’s difficult for a male to undergo spermatogenesis. 01:22 And so therefore – well look for – A different physiology question of this would be if you have a male that’s in different temperatures, right? Environments. 01:31 And so therefore, may not be the most conducive to spermatogenesis Even for example, bicyclists and what do they do? They sit on that seat for hours and hours and hours. 01:42 And that disrupts proper spermatogenesis. 01:45 No joke. 01:46 Meaning to say that even lifestyle and the way that you lead it could have serious sequelae or consequences. 01:53 Presents in 1% of boys at 1 year of age. 01:56 With increased occurrence in premature or even Klinefelter. 02:00 Our topic cryptorchidism, undescended testis, 1 in 1. 1% in 1 year of age. 02:05 Klinefelter is big. 02:07 What does your patient with Klinefelter look like? Picture that. 02:09 Patient, please? Long arms, long legs, maybe perhaps gynecomastia, but the jaw looks like a male. 02:19 Testosterone levels are normal in unilateral cryptorchidism due to unaffected Leydig cells. 02:26 So you can have the other scrotum with it’s Leydig cells in which -- You tell me as to what hormone acts upon the Leydig cell. 02:33 Good. LH. 02:34 Responsible for testosterone synthesis. 02:37 But descreased in bilateral, obviously. 02:39 So here, if you have bilateral undescended testis, then the Leydig cells are not able to properly perform. 02:45 So therefore, you would have suboptimal levels of testosterone. 02:49 Is that understood? That’s important. 02:52 Inhibin B levels are depressed with increased LH and FSH and there’s increased risk of germ cell tumors. 02:59 These two bulletpoints are very, very important for you to know. 03:02 If you don’t have proper – I’m going to bring you back to physiology real quick – tell me as to where inhibin B comes from in the male? Good. 03:11 Sertoli cells. 03:12 So if you don’t have proper descent of the testis, then the sartoli cells are not able to properly release inhibin B. 03:19 Inhibin B works on, if you remember, the hypothalamo–pituitary axis and so therefore, normally it inhibits. 03:27 So if you don’t have the inhibin B, you’re going to increase your gonadotropin hormones, increase LH and FSH. 03:33 Make sure you know the feedback. 03:35 Every little point here has a story. 03:39 And the last little point with cryptorchidism is the fact that your male is now prone to -- the most common family of testicular tumors are germ cell tumors. 03:50 Of all the germ cell tumors, which is the most common? Seminoma.
About the Lecture
The lecture Cryptorchidism by Carlo Raj, MD is from the course Male Reproductive System Diseases.
Included Quiz Questions
Which statement regarding cryptorchidism is CORRECT?
- It is associated with an increased risk of germ cell tumors.
- It is associated with an increased risk of squamous cell cancer.
- Prematurity significantly decreases the risk.
- It is present in 10% of 1-year-old boys.
- Testosterone levels are always abnormal.
In which condition are plasma testosterone levels decreased?
- Cryptorchidism of both testicles
- Cryptorchidism of one testicle
- Hypospadias
- Epispadias
- Priapism
Author of lecture Cryptorchidism

Carlo Raj, MD
Customer reviews
1,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
1 customer review without text
1 user review without text
