Playlist
Show Playlist
Hide Playlist
Hypothyroidism

-
Slides Hypothyroidism EndocrinePathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
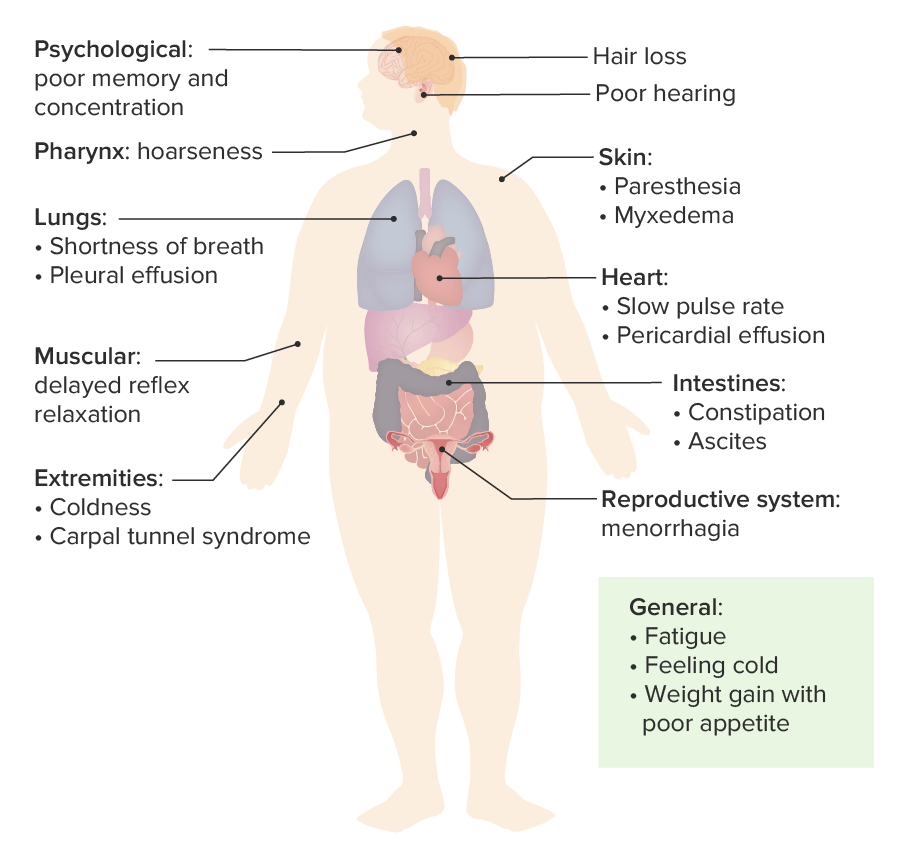
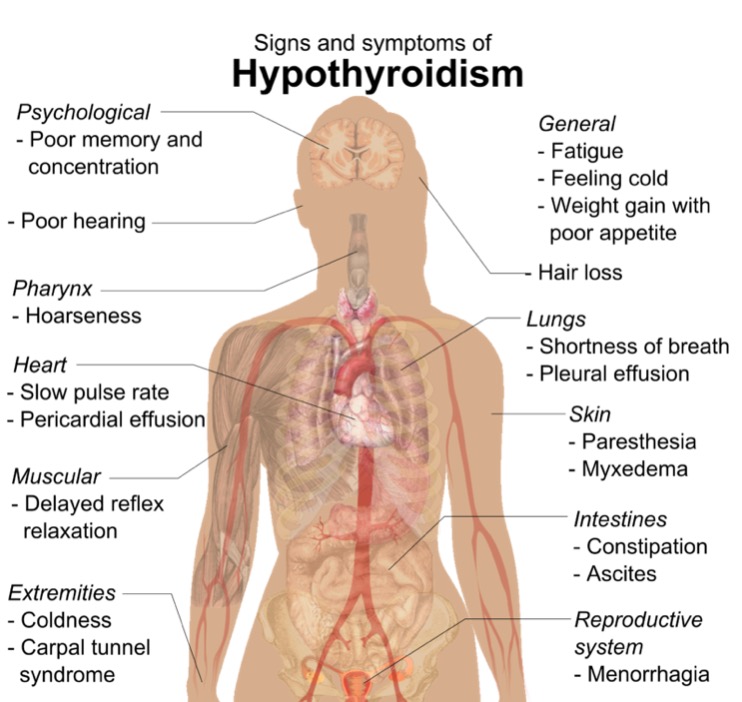
00:01 Congenital Hypothyroidism is a condition characterized by a deficiency of thyroid hormone at birth. 00:07 It was Historically referred to as “cretinism,” a term no longer used due to its inaccuracy and negative connotations. 00:15 Iodine lacking in a pregnant woman resulting in decreased thyroid hormone nourishment to the foetus; enzymatic deficiency in the fetal thyroid gland resulting in lack of T3, T4. 00:31 Failure of the thyroid gland to properly develop in the neck where it should belong or anti-thyroid antibodies from the mother attacking the fetal thyroid, therefore may result in hypothyroidism. 00:47 Over 95% of newborns with congenital hypothyroidism actually show few or no signs at birth. This can be quite surprising, but there are two main reasons for this. Maternal thyroxine can cross the placenta to the child, and some infants may have a small amount of functional thyroid tissue. 01:06 Both of these may allow partial compensation and mitigate the severity of symptoms early on. 01:12 However, as the infant grows and the demand for thyroid hormone increases, this compensation is no longer sufficient, and if untreated, characteristic symptoms and signs begin to emerge. 01:26 For easy recall of these signs and symptoms, we use the mnemonic of the "6 Ps," which are: Pot belly: or distended abdomen due to decreased muscle tone and accumulation of substances, like mucopolysaccharides, within the gut. 01:42 Pallor: not just because of anemia, but also due to the myxedematous skin changes. 01:49 Puffy face: due to facial myxedema. 01:52 Protruding umbilicus: often due to an umbilical hernia. 01:56 Protuberant tongue: or macroglossia, which can contribute to feeding difficulties. 02:02 Prolonged jaundice: particularly unconjugated hyperbilirubinemia, related to decreased metabolism of bilirubin. 02:10 Other important signs include lethargy and hypotonia. The long-term consequences of untreated congenital hypothyroidism are serious and irreversible. 02:21 Without timely treatment, several significant and irreversible changes can occur: Thyroid hormones are essential for central nervous system development, particularly during the first few months after birth. A deficiency can lead to severe intellectual disability. 02:37 Thyroid hormones also influence bone growth and development. 02:41 Without adequate levels, children can experience delayed skeletal maturation, leading to short stature. 02:48 This is a physical manifestation that is often readily apparent. 02:52 Additionally, hypothyroidism can lead to hypotonia, which may affect a child’s motor skills and physical abilities. 03:01 The physical effects of congenital hypothyroidism due to iodine deficiency are demonstrated in the photograph on the right. 03:09 The takeaway here is the critical importance of newborn screening programs, which enable healthcare providers to detect the condition early and start treatment before these irreversible effects take hold Let’s talk about myxoedema and hypothyroidism and this would be for an adult. 03:26 Take a look at the face in this patient on the left with hypothyroidism. 03:31 The patient was then treated with synthroid. 03:35 Upon administration, you’ll notice that months afterwards, on your right, the same patient, the puffiness on the face has now become diminished. 03:45 The myxoedema subsides upon administration of levothyroxine in a patient with hypothyroidism. 03:52 Would you expect such puffiness in a patient with Graves’ disease? Not at all, the myxoedema that you find in Graves’ disease will be located most likely pretibial. 04:05 Remember I showed you and have shown you pretibial myxoedema along with dermopathy of Graves’? This however is myxoedema in hypothyroidism. 04:18 Broadening, coarsening facial features, lower pitched voice… what is myxoedema? It’s the accumulation of Gags… glycosaminoglycans and hyaluronic acid in the subcutaneous tissue The increased dermal glycosaminoglycans trap water, giving rise to skin thickening without pitting Now, I will now mention our last topic in myxoedema that’s upcoming and that would be myxoedema coma which is the… that name will be modified in due time, but please, know it now. 04:52 There’s been worst case hypothyroidism where your patient has not gone into a coma only after hypothyroidism is completely and relentlessly taken its course in your patient. 05:07 Myxoedema coma occurs in patients with long standing, untreated, relentless, severe hypo… hypothyroidism, not hyper. 05:20 Often precipitated by stress such as systemic illness or surgery. 05:25 Presentation: hypothyroidism with mental status changes to the point of absolute stupor, seizures and coma and perhaps death. 05:34 Mortality… no joke, look at this 50 percent! You want to do everything in your power to prevent your patient with hypothyroidism ever getting into such as state because you’ll probably never get them back. 05:50 Topic now goes to subclinical hypothyroidism. 05:52 The last time we talked about this was subclinical… well, the related topic earlier was subclinical hyperthyroidism. 06:05 Subclinical hyperthyroidism is extremely common in our society. 06:10 What subclinical means is the fact that the patient is not exhibiting or expressing overt symptoms of hypo or hyperthyroidism, thus you call it subclinical. 06:23 On the wards and on your boards, do not get subclinical confused with sub-acute; one has nothing to do with the other. 06:32 Subclinical means that the patient appears as though, on biochemical exam, that there is a normal free T4 with a slight elevation of TSH, but the patient is not presenting with severe hypothyroid symptoms… mild. 06:49 15 to 20 percent of individuals over the age of 60 will be suffering from subclinical hypothyroidism, but they don’t even know it. 06:57 Usually caused by a Hashimoto-type of event.
About the Lecture
The lecture Hypothyroidism by Carlo Raj, MD is from the course Thyroid Gland Disorders.
Included Quiz Questions
What is the most common cause of congenital hypothyroidism in the world?
- Lack of iodine in the pregnant woman's diet
- Excessive exposure to sunlight during pregnancy
- Fetal thyroid enzyme deficiency
- Thyroid dysgenesis
- Consumption of certain medications during pregnancy
In an infant with congenital hypothyroidism who is not treated, what are the typical signs and symptoms that can be seen after 2 months? Select all that apply.
- Pot belly
- Rapid weight loss
- Pallor
- Puffy face
- Protruding umbilicus
What must be accumulated to produce myxedema in hypothyroid patients?
- Glycosaminoglycans
- Lymphocytes and eosinophils
- Albumin and plasma
- LDL and fatty acids
- Thyroid hormone bound to TBG
Myxoedema coma occurs in patients with...?
- Long standing, untreated, severe hypothyroidism
- Newly diagnosed, mild hypothyroidism
- Acute, viral thyroiditis
- Over-treatment with synthetic thyroid hormones
- Chronic, untreated hyperthyroidism
What best describes subclinical hypothyroidism?
- Elevated TSH with normal free T4
- Elevated bound T4 with normal free T4
- Normal TSH with low free T4
- Elevated TBG with normal TSH
- Low free T3 with normal free T4
Author of lecture Hypothyroidism

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
