Playlist
Show Playlist
Hide Playlist
Corynebacterium Diphtheriae


-
01-04 Corynebacterium.pdf
-
Download Lecture Overview
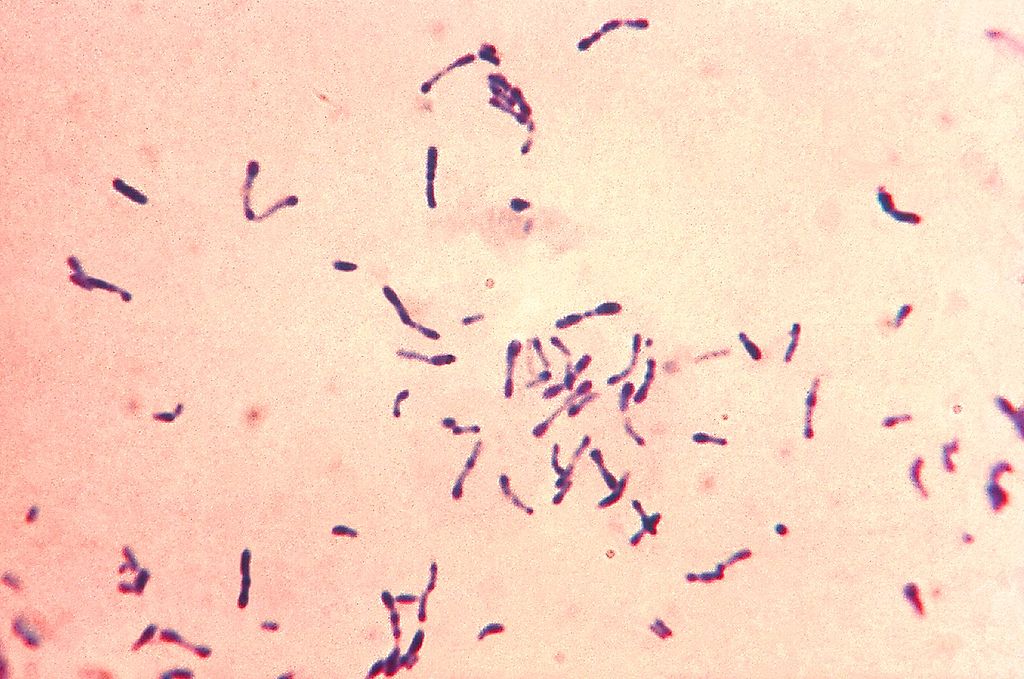
00:01 Corynebacterium diphtheria; a bacteria. 00:04 Corynebacterium are gram-positive bacillus which are aerobic and non-sporm - spore forming rods with meta-chromatic granules which you can see if you focus closely on the slide with the pictures. 00:20 In addition, the organisms appear club shaped, you can see a prominent end of each end of the bacillus. 00:27 If grown on Löffler medium, they appear as gray to black colonies on the Tellurite agar. 00:36 Now, why is Löffler medium important? Because Dr. Loeffler was one of the discoverers of corynebacterium diphtheria. 00:44 Corynebacterium are transmitted by aerosol droplets, they are very typically present in the respiratory flora and it does not take much for them to be sneezed or coughed. 00:55 Also, if there's a break in the skin with somebody who has a cutaneous infection with diphtheria, it can be transmitted in that way as well. 01:06 There are several important clinical diseases associated with diphtheria. 01:11 The first is the classic or the respiratory diphtheria which causes a pseudomembranous pharyngitis. 01:18 Pseudomembrane; this is not a true membrane or tissue which is found in the pharynx but it is created by all of the necrotic and inflammatory debris which coats the inner part of the pharynx. 01:32 Many times, it also covers and crosses or blocks the pharynx. 01:38 So patients with true respiratory diphtheria, due to the pseudo-membrane are unable to breathe because their windpipe; their trachea is completely blocked by that mechanism. 01:51 In addition, they may have severe lymphadenopathy which you see in the picture on the lower right. 01:58 The patient has what looks like a bull neck that is really a reference to a very swollen neck due to very significantly swollen lymph nodes in the anterior and the posterior cervical chains. 02:11 The other form of diphtheria though is wound or cutaneous diphtheria. 02:16 And this starts initially in a very minor fashion as a small papule; a small red bump, which then develops into the picture you see in the upper right as a chronic nonhealing ulcer. 02:27 Rarely, both of these illnesses can present and progress to a systemic toxemia in which the patients develop multiorgan disease or damage to distant organs including the myocardium causing cardiac failure, arrhythmias, neuropathy, and then renal tubular necrosis causing kidney failure. 02:50 Pathogenesis. How does this illness - or how does this organism cause illness? It starts in the form of a bacteriophage, a lofty little bacteriophage which introduces itself into the DNA of the organism and that encodes a diphtheria exotoxin. 03:11 The toxin is really the major cause of the disease in dipthereia because it ribosylates ADP present in the elongation factor. 03:22 That doesn't sound too awfully bad until you realize that elongation factor and especially elongation factor 2 is critical for the elongation of protein chains. 03:33 So if you inhibit its function as happens with diphtheria exotoxin, the patient's cells are unable to protein synthesize. 03:42 They're unable to do the normal works of life. 03:45 And so that causes cell death and the secondary clinical manifestations. 03:50 How do we make the diagnosis? Well, a clinical diagnosis is probably the most likely one, but you'll be - also expected to know how this might be done in the laboratory. 04:02 Now let's discuss the lab diagnosis, definitive diagnosis of the theory that requires a culture of corynebacterium diphtheriae from respiratory tract secretions or cutaneous lesions, as well as a positive toxin assay. 04:15 The presumptive diagnosis can be made with a gram stain that shows gram positive rods typically appearing as club shaped rods in a zigzag period, or what may be described as a Chinese character distribution. 04:27 For testing purposes, remember, you may also see monochromatic granules when staining with aniline dyes or lafleur's media. 04:35 Further confirmation can be ascertained by additional testing for exam purposes. 04:40 Remembering this organism is catalase. 04:42 Positive is the most important. 04:44 There are several methods to test for the diphtheria toxin, including a rapid test and a PCR test that identifies the gene. 04:51 It should be noted, however, that a negative PCR test is very sensitive at excluding a diphtheria diagnosis. 04:58 Now, instead of delaying treatment while awaiting these testing results, a high clinical suspicion is important and is all that is required to begin. 05:06 Administration of the anti toxin. 05:08 Do not wait. 05:10 Finally, any cases of clinical disease caused by corynebacterium diphtheria toxin must be reported to your local and regional health department. 05:19 A positive laboratory test without clinical symptoms can be considered only to be a carrier infection, which does not require reporting. 05:27 So, what about that prevention? Well, diphtheria has been a component of the diphtheria pertussis toxin vaccine for a very long time and it is very successful, but a booster is necessary. 05:42 If a patient however is not protected; does not have that immuno protection from vaccine and they developed disease related to diphtheria. 05:52 Then tetanus and diphtheria immunoglobulin can be used to neutralize the toxins of the actual disease. 06:01 So in treating a patient with diphtheria, penicillin is the typical antibiotic which is most successful. 06:07 However, erythromycin also works for those who are penicillin allergic. 06:12 We would also however use antibiotics to treat close contacts of the index patient because they may have acquired disease via that respiratory or cutaneous mechanism. 06:23 So diphtheria, hopefully is a very rare infection to encounter, but it is an important organism to remember and to understand. 06:32 Again, keeping in mind that it looks like metachromatic clubs under the microscope and that it can cause a pseudomembrane in the airway of a patient who has respiratory diphtheria.
About the Lecture
The lecture Corynebacterium Diphtheriae by Sean Elliott, MD is from the course Bacteria.
Included Quiz Questions
The typical shape of Corynebacterium diphtheriae is which of the following?
- Club-shaped
- Needle-shaped
- Spherical
- Polyhedral
- Bullet-like
Which of the following forms of pharyngitis would you expect to encounter in a patient presenting with respiratory diphtheria?
- Pseudomembranous pharyngitis
- Catarrhal pharyngitis
- Ulcerative pharyngitis
- Atrophic pharyngitis
- Purulent pharyngitis
Which of the following terms best describes the characteristic granules present in Corynebacterium diphtheriae?
- Metachromatic
- Panchromatic
- Isochromatic
- Monochromatic
- Apochromatic
Which of the following refers to the type of vaccine used for the prevention of diphtheria?
- Toxoid
- Live attenuated
- Killed/inactivated
- Subunit
- Recombinant
Author of lecture Corynebacterium Diphtheriae

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
