Playlist
Show Playlist
Hide Playlist
Colonic Ischemia with Case

-
Slides Gastroenterology 09 Disorders Large Intestine II.pdf
-
Reference List Gastroenterology.pdf
-
Download Lecture Overview
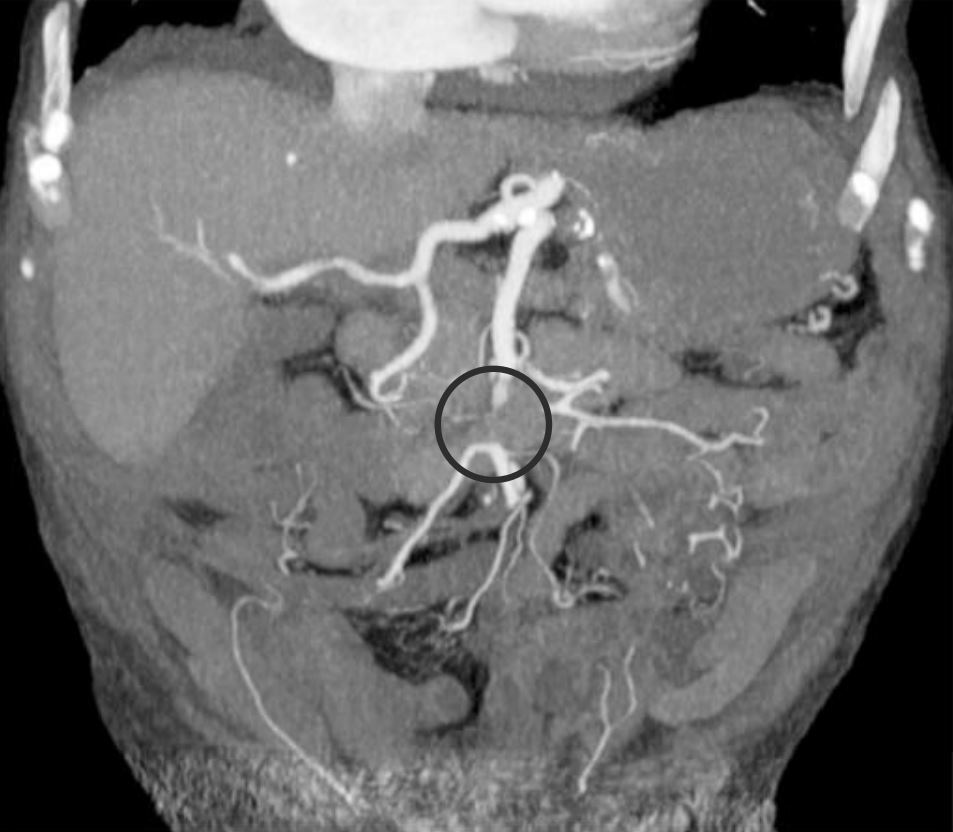
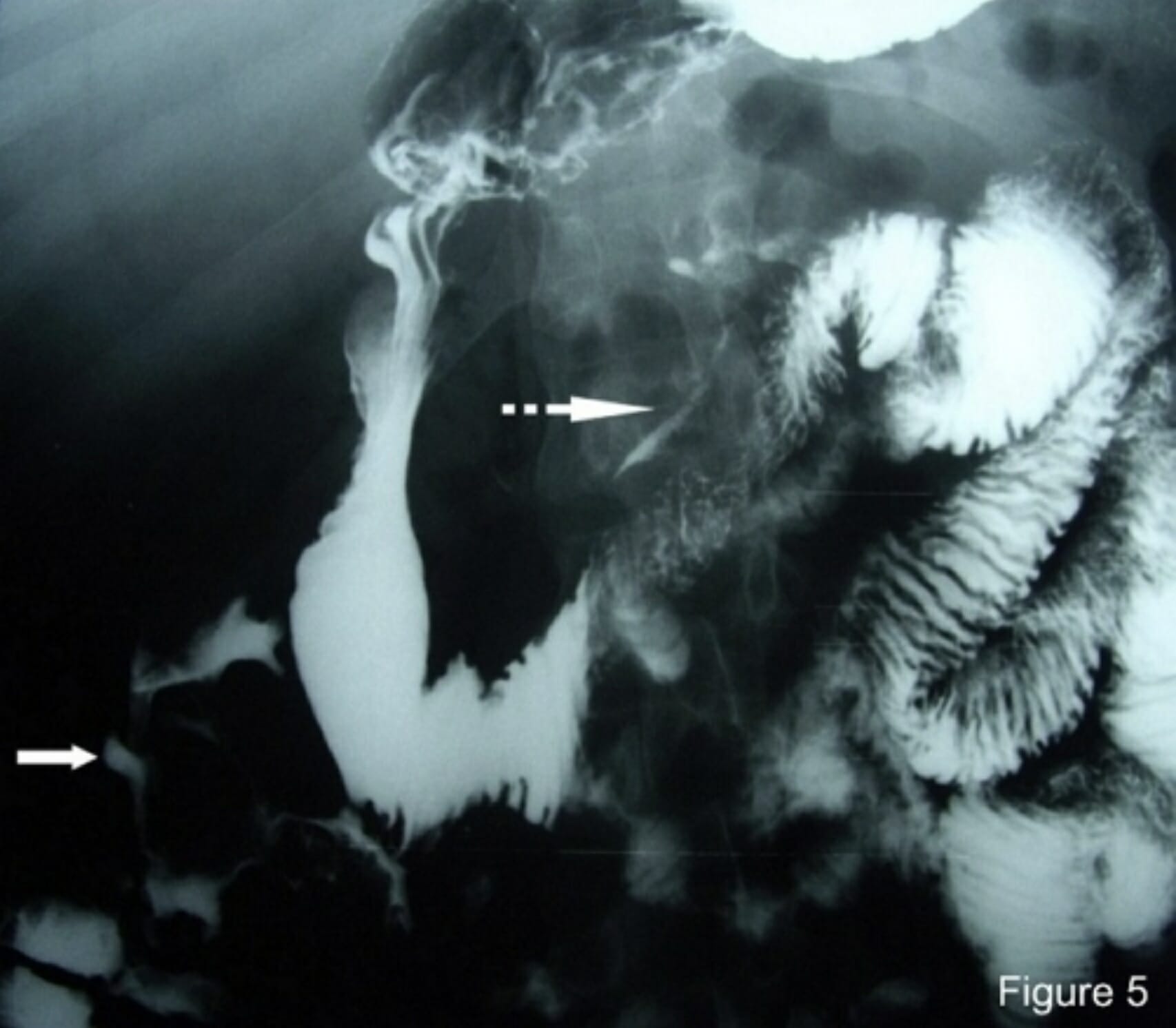
00:01 We'll move on to our next case now. 00:03 We have a 69-year-old woman with coronary artery disease who was admitted to the ICU for septic shock due to pneumonia. 00:11 She has started on broad spectrum antibiotics and norepinephrine. 00:15 On hospital day 3, she developed sudden-onset crampy abdominal pain And a few hours later, she develops hematochezia. 00:24 Vitals are notable for blood pressure of 89/55 and a pulse of 110 On abdominal exam, she has tenderness on the left side without rebound or guarding. 00:35 Her rectal exam confirms bright red blood. 00:38 Labs show hemoglobin of 8 g/dL, leukocyte count of 20,000/uL and lactate of 8 mmol/L. 00:45 CT of the abdomen shows edema and thickening of the ascending colon. 00:50 So what is the most likely diagnosis? So we'll point out that she has new abdominal pain and bright red blood per rectum or hematochezia and she's a patient with hemodynamic instability. 01:03 Her physical exam localizes to the left side of her abdomen with confirmed hematochezia on rectal exam. 01:10 And she has a high lactate with a high white count. 01:14 In addition, her CT imaging is concerning and we'll go over that next. 01:20 So, she most likely has colonic ischemia. 01:23 This is what occurs when there is lack of perfusion to the bowel wall leading to an infarct of the bowel. 01:31 Recall that this tends to occur In an areas with limited collateral circulation. 01:36 So we'll have to go back to our anatomy here on the right and remember that there are two areas that we call watershed areas where there is limited collaterals flow between the large vessels that supply the colon. 01:49 So the first area is the splenic flexure, which is the area between the SMA and the IMA The second area that’s prone to develop with ischemia is the rectosigmoid junction which is between the IMA and the hypogastric arterial system. 02:06 So patients may present with sudden crampy abdominal pain. 02:10 They often have hematochezia, an urgent desire to defecate and they may have elevated lactate and elevated white counts. 02:21 The diagnosis is made mostly clinically however he may also do CT abdomen with IV contrast, or colonoscopy if the diagnosis remains unclear. 02:33 Treatment consists of primarily supportive care, doing bowel rest to prevent further ischemia to the area, and surgical resection if bowel necrosis has occurred or if the patient has now developed peritonitis. 02:51 So there are common risk factors for developing colonic ischemia. 02:55 The number one factor is atherosclerotic disease which already limits blood flow to the area, hypotension, strenuous physical activity which can divert blood flow to other areas of the body, vasoconstricting medications or drugs that also prevent blood flow to the area. 03:13 or thrombophilia which is either inherited or acquired ability to develop blood clots. 03:22 So now let's return to our case. 03:24 We have a 69-year-old woman with new-onset abdominal pain and hematochezia with hemodynamic instability. 03:33 Her exam and labs are concerning for some intraabdominal pathology and her CT imaging shows findings consistent with bowel ischemia. 03:43 So the most likely diagnosis here is colonic ischemia. 03:49 Thank you very much for your attention.
About the Lecture
The lecture Colonic Ischemia with Case by Kelley Chuang, MD is from the course Disorders of the Small and Large Intestines.
Included Quiz Questions
Which of the following is the most common area affected by colonic ischemia?
- Splenic flexure
- Ascending colon
- Transverse colon
- Rectum
- Sigmoid colon
Which of the following is the best next step if the diagnosis of colonic ischemia is unclear after an abdominal CT scan?
- Colonoscopy
- Abdominal ultrasonography
- Abdominal X-ray
- CT angiography
- Surgery
Author of lecture Colonic Ischemia with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
