Playlist
Show Playlist
Hide Playlist
Clinical Question: Cortical, Subcortical or Brainstem Localization?

-
Slides Stroke and intracranial hemorrhage.pdf
-
Download Lecture Overview
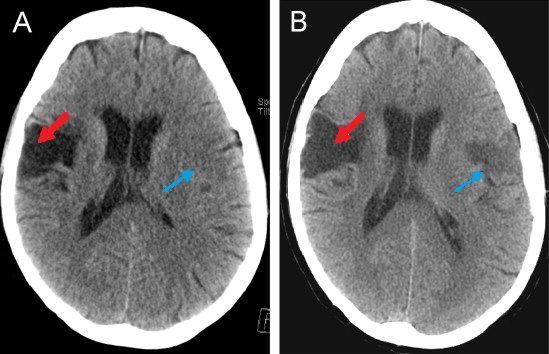
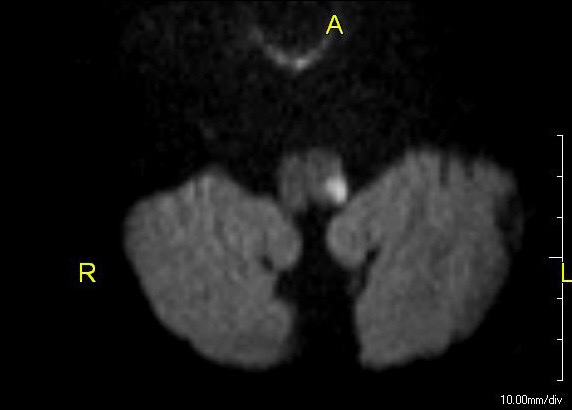
00:01 The second thing we ask when evaluating a stroke patient is, is this stroke, cortical, subcortical or brainstem in localization? When we're looking at the patient and examining the patient, the findings that we see help us to localize to a certain territory and can hone in on a blood vessel that we're concerned about or the likelihood of recovery with intervention. 00:23 So let's walk through some of those regions. 00:26 Cortical avascular territories that supply the cortex include the ACA, MCA, PCA, and both of those watershed territories, ACA-MCA (Watershed) and MCA-PCA (Watershed). 00:39 Vascular territories for a subcortical localization are basal ganglia, thalamocapsular, and the internal capsule specifically. 00:47 And then in brainstem we think about strokes affecting the midbrain: pons, medalla and the cerebellar fibers. 00:55 So let's walk through each of those localizations, each of those territories and understand better how patients will present. 01:02 And let's start with a cortical localization. 01:05 What does it look like to have a cortical stroke? What do we see on patients and what's going to tip us off to those arteries ACA, MCA, PCA and the watershed territories? Well first, cortical strokes imply a large territory, both the subcortex and frequently the cortex are involved. 01:24 And that suggests and tips us off that we should be initially concerned about an embolic phenomenon. 01:30 Large territory strokes come from a very proximal clot, the proximal blood vessels are large and so we're looking for a large clot, typically of an embolic source, or sometimes intracranial atherosclerosis that's developed over a long period of time. 01:47 These patients are at risk for recurrence if it is embolic, so we really want to diagnose the embolic phenomenon and intervene to prevent that from worsening. 01:56 And patients with large territory strokes affecting the cortex are at risk for swelling, brain swelling, mass effect, increased intracranial pressure, and herniation. 02:07 The signs of a cortical stroke are cortical signs. 02:10 Language or aphasia is a cortical finding. 02:13 And so aphasia suggests cortical localization specifically in the MCA territory, either the frontal lobe for expressive aphasia, the temporal lobe for receptive aphasia, the arcuate fasciculus, if repetition is involved. 02:27 Patients may have gaze preferences, the frontal eye fields are located in the cortex of the frontal lobes and problems strokes affecting the frontal eye fields can cause patients to prefer to look to one side or the other. 02:39 Neglect is a parietal cortical function, and patients who present with prominent neglect will worry about pride or involvement of their stroke. 02:47 Cortical sensory findings, stereognosis or graphesthesia are also cortical findings suggestive of a parietal localization. 02:56 Personality changes from cortical frontal dysfunction, and homonymous hemianopia is an occipital cortical function where we would worry about about post your circulation, a cortical localization. 03:11 When we think about cortical stroke, strokes involving those signs and suggestive of a cortical process, we are worried about large and medium size vessel occlusions. 03:22 And this can point us to the etiology, as well as have implications for treatment. 03:27 So the three things we worry about is causing cortical strokes are emboli which cause proximal large vessel occlusion or LVO, large vessel occlusion. 03:37 Thrombotic processes, large and medium size vessel occlusion that occur in patients who have significant risk factors or long term develop a development of atherosclerosis and thromboembolic disease. 03:49 These would be areas of clots on the carotid arteries that embolize distally to the large and medium sized vessels, again causing occlusion. 03:58 So when we evaluate patients if we're worried about an embolic phenomenon, we want to evaluate the heart. 04:04 Cardioembolisms or embolisms that arise from the heart, and we look at the heart with a transthoracic echocardiogram. 04:10 We do an EKG or telemetry to evaluate for paroxysmal atrial fibrillation, which could give rise to cardioembolism and we consider anticoagulation. 04:20 If we're worried about thrombotic disease or also thromboembolic disease, we need to evaluate for a source or a site of the thromboembolism. 04:28 We look at the carotid arteries with carotid ultrasound or angiography of the carotid arteries. 04:34 And we want to manage patients risk factors with risk factor modification, reducing high cholesterol, managing diabetes and reducing high blood pressure. 04:45 What about subcortical localizations? What are subcortical strokes and what's tips us off that we're dealing with a subcortical phenomenon? These strokes typically present with hemibody motor or sensory symptoms without cortical involvement. 04:59 So the cortical signs we just discussed, we don't see with these strokes. 05:03 Instead, we see hemiparesis or hemiplegia, hemianesthesia or hemisensory loss, and those would point us to a subcortical localization. 05:13 In addition, there are some rare syndromes that are subcortical syndromes. 05:17 Ataxia-hemiparesis. 05:19 That's a patient who can't move one side of the body, has a weak arm and leg with superimposed ataxia, and that implies a subcortical, typically thalamocapsular, internal capsule, or a thalamic and internal capsule stroke. 05:33 We can see movement disorders from strokes in the substantia nigra, and sometimes globus pallidus, and other basal ganglia structures. 05:40 Strokes in the thalamus can cause a severe and debilitating thalamic pain syndrome, which is rare but very important. 05:47 And we can see thalamic aphasia is typically aphasia is a cortical sign. 05:51 But in selective, deep thalamic strokes, particularly left sided thalamic strokes, we can see aphasia from the thalamus. 05:59 The thalamus is the relay center to all areas of cortex and that start to contribute to the reason for aphasia and a thalamic pathology and specifically in stroke. 06:11 The subcortical strokes importantly are called lacunar syndromes. 06:15 And that's because these strokes typically develop from a lacunar process, a small blood vessel, a small vascular blood vessel that develops clots, and typically we think about this in patients who have long standing hypertension. 06:30 So when we're evaluating the subcortical strokes, we think about small vessel etiology. 06:35 The most common cause of a small vessel stroke is a lacunar stroke. 06:39 And we also think about thrombotic disease or atherosclerotic disease. 06:43 Lacunar strokes are heavily linked to long standing hypertension, that long history of high blood pressure results in thickening of the tunica media reduction in the lumen size within those small vessels. 06:56 And eventually, we can see closure and blockage of the small vessels. 07:00 Management of hypertension is critical in lacunar strokes. 07:04 For thrombotic strokes or atherothrombotic strokes, we think about managing stroke risk factors. 07:10 So again, the localization of the stroke can drive us to the etiology, tell us what the favorite etiology is and help us with managing the patient. 07:19 What about the brainstem? The brainstem is a really large place, there's a lot going on with a lot of function. 07:25 How do we localize a stroke to the brainstem and then use that to evaluate the patient? Well, there are a few hallmarks of brainstem strokes and you can see those here. 07:35 One is crossed findings. 07:38 And that's one symptom or sign on one side of the body. 07:41 And that same symptom or sign or sometimes a different symptom or sign on the other side of the face. 07:46 So weakness on one side of the face and weakness on the opposite side of the body. 07:50 Sensory loss on one side of the face and sensory loss on the opposite side of the body. 07:55 Those crossed findings point squarely to a brainstem stroke. 08:00 Patients may also present with impaired consciousness, this is one of the only times that stroke will cause impaired consciousness. 08:08 That's because what allows us to be consciousness. 08:10 Conscious is two things. 08:11 The reticular activating system which needs to work in the brainstem and needs to light up the bilateral hemispheres. 08:19 Strokes are frequently not big enough in the bilateral hemispheres are usually don't affect the bilateral hemispheres to cause launches loss of consciousness from a hemispheric stroke. 08:28 But the reticular activating system is a small area in the brainstem. 08:32 And deep central pontine perforator strokes can affect the reticular activating system and present with impaired consciousness. 08:41 And in addition, we can think about brainstem strokes both longitudinally and cross sectionally. 08:47 Longitudinally, we can divide them into strokes that affect the midbrain, pons and medalla. 08:53 And knowing both the cranial nerves and the white matter tracks that course through there can help us to localize. 08:59 Cross sectionally, we can divide brainstem strokes into ventral findings and dorsal findings. 09:05 And using that combination, we can localize precisely to where the patient's stroke is originating from. 09:12 So let's look at that a little bit more in depth. 09:16 First of all, brainstem strokes are posterior circulation in etiology, so we want to interrogate the posterior circulation. 09:23 Vessel imaging is critical. 09:26 And typically we don't stop at ultrasonography but extend into CT angiography or MR angiography to definitively assess the vertebral arteries and the basal or artery and all of its blood supply. 09:39 We need to evaluate patients for any potential basal or artery thrombosis. 09:44 Thrombosis in the basilar artery is a medical emergency and must be evaluated and managed acutely. 09:52 Let's look at some of the brainstem presentations and signs. 09:56 Quadriparesis or motor loss in all four limbs. 10:00 If it includes the face, implies a vascular territory that is above the pons and involves the pons or above the facial fibers, the motor function of the face comes out in the pons or exits the brainstem and the pons. 10:15 And so if the face is involved, we worry about pons or above. 10:18 If there's quadriparesis weakness in all four limbs or quadriplegia, inability to move all four limbs that doesn't involve the face. 10:26 We think about below the pons, the medulla or the upper part of the cervical cord. 10:33 We can also see hemiparesis or hemibody symptoms. 10:37 Hemibody symptoms imply loss on one side of the nervous system or the other. 10:43 If the symptoms in the face are the same side as the symptoms in the body, again, we think about that problem, that pathology, that stroke involving either the pons or above the pons. 10:55 If there are crossed findings, findings on one side of the face and the opposite side of the body that would be a lesion at the level of the pons. 11:02 And if the face is spared, we worry about lesions that are below the pons. 11:06 So the involvement of the face is critical for localizing that stroke to above at or below the pons. 11:14 And here you can see an example of those crossed findings. 11:17 Here we see symptoms on the left side of the face and the right side of the body, which implies stroke or pathology at the level of the pons or in somewhere in the brainstem. 11:30 Other brainstem findings that we can see. 11:32 Again, decreased level of consciousness sometimes nausea and vomiting with specific posterior circulation or medullary pathology hiccups, abnormal respirations. 11:42 Oropharyngeal weakness from lower cranial nerve dysfunction. 11:45 Vertigo and tinnitus, eye movement abnormalities either diplopia, dysconjugate gaze, gaze deviation or frank gaze palsy, the inability to move the eyes in one direction or the other. 11:57 The brainstem controls all the cranial nerves and so we can see cranial nerve dysfunction.
About the Lecture
The lecture Clinical Question: Cortical, Subcortical or Brainstem Localization? by Roy Strowd, MD is from the course Stroke and Intracranial Hemorrhage.
Included Quiz Questions
What test(s) is (are) used to evaluate for a cardiac cause of an embolic stroke?
- Echocardiogram
- CT scan
- MRI
- CTA or MRA
- Electrocardiogram (ECG)
What would be a clinical manifestation of a stroke in the substantia nigra area of the brain?
- Movement disorder
- Hemibody sensory loss
- Hemiplegia of the ipsilateral side
- Hemiplegia of the contralateral side
- Ataxia
Cranial nerve symptoms of oropharyngeal weakness, eye movement abnormalities, and vertigo are due to a stroke in what area of the brain?
- Brainstem
- Thalamus
- Left cerebral cortex
- Right cerebral cortex
What is the reason for localizing the area affected by a stroke?
- To manage the probable etiology of the stroke
- To decide if thrombolytic therapy is indicated
- To evaluate the risk factors for a stroke
- To determine if diabetes is the cause of the stroke
- To determine if high cholesterol is the cause of the stroke
What is the biggest risk factor for a lacunar or small vessel stroke?
- Long-standing hypertension
- Uncontrolled diabetes
- Smoking
- Hyperlipidemia
- Obesity
Author of lecture Clinical Question: Cortical, Subcortical or Brainstem Localization?

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
