Playlist
Show Playlist
Hide Playlist
Group 3: Potassium Channel Blockers – Antiarrhythmic Drugs

-
Slides Group 3 Potassium Channel Blockers Antiarrhythmic Drugs.pdf
-
Reference List Pharmacology.pdf
-
Download Lecture Overview
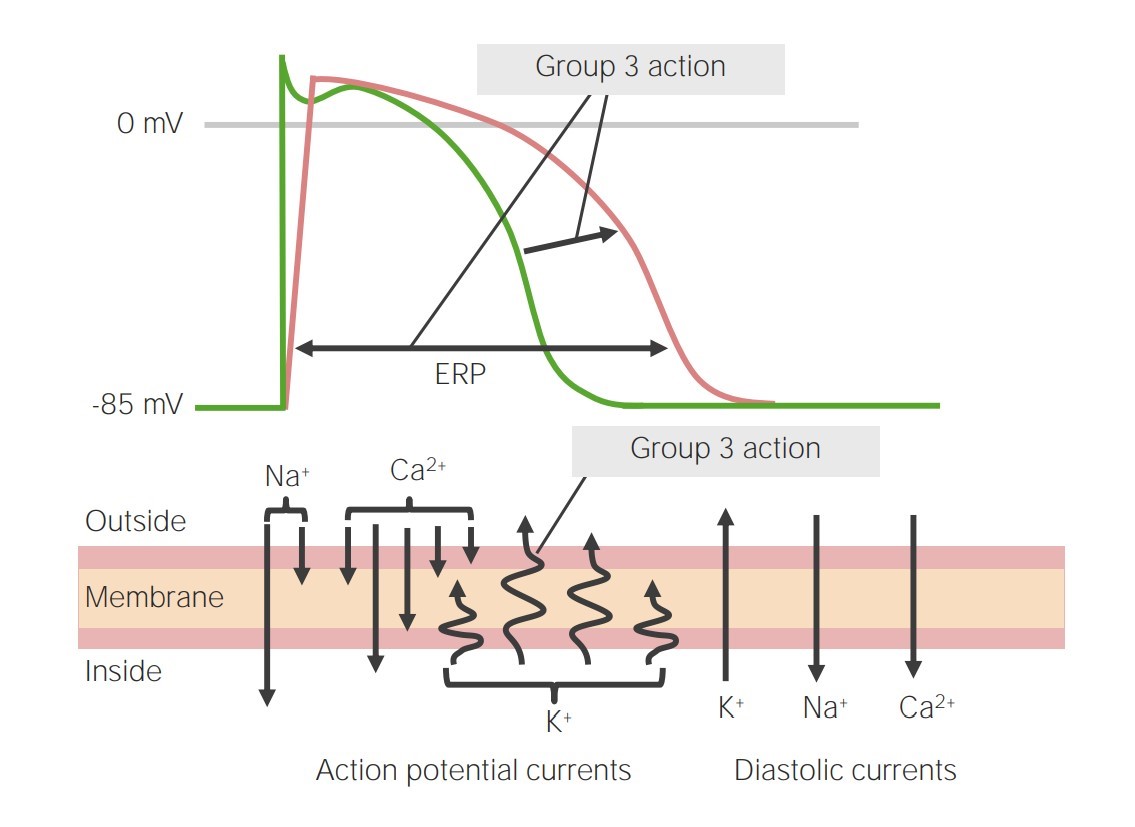
00:01 The group 3 antiarrhythmics are quite complex, but they are actually a lot of fun to use, a lot of fun to administer, and a lot of fun to learn about. 00:09 So these are potassium channel blocker active agents. These channels are responsible for repolarizing the membrane. 00:19 Now, it includes medications that "cross" into other classes as I mentioned before. 00:24 It prolongs the action potential and it also increases the QT interval on the electrocardiogram. 00:31 The most important thing that I want you to remember is that this drug increases the effective refractory period. 00:37 And that reduces the response to atrial tachycardia. 00:42 Now, the classic drugs in the group 3 is ibutilide, prototypical drugs. 00:47 Now, sotalol is a beta blocker but it's also a class 3 antiarrhythmics. 00:52 It's a chiral mixture of two different types of sotalol. So, chiral means mirror image. 01:00 So for example, my left hand is a chiral image of my right hand. 01:07 Amiodarone and dronedarone are class 3 antiarrhythmic drugs. 01:12 In fact, amiodarone is probably the most commonly used antiarrhythmic today. 01:17 And I would argue that it is the most effective antiarrhythmic out there. 01:20 It blocks the potassium current, as well as the sodium and calcium current. 01:25 And it also has some beta blocking ability. So, you can see that drugs in this class cross classes. 01:31 They are hard to classify, but let's leave it in the group 3 drugs. 01:36 I want to talk specifically about amiodarone for a moment because you're going to encounter these patients on amiodarone all the time, and it's going to be a big part of the pharmacology cardiology lectures, and it's going to be a big part of your exam. 01:50 So, toxicity is important to know. One of the things that we see with amiodarone toxicity is pulmonary fibrosis. 01:57 And here you can see a chest X-ray, classical for amiodarone fibrosis. 02:02 These are multiple areas of microcrystalline deposits. It causes pulmonary fibrosis because the lung is reacting to those crystalline deposits. 02:13 The other thing that you see is a similar kind of destruction in the thyroid gland. 02:17 A similar kind of dysfunction and destruction in the nerves, so you get paraesthesias and tremor. 02:24 And you can get ocular or corneal deposits. We call that corneal verticillata. 02:31 So, let's just slow down, and we will go over this in detail. 02:35 So, amiodarone is the most commonly used, most effective antiarrhythmic out there. 02:40 Remember, once again, it blocks the potassium, the sodium, and the calcium channels. 02:46 And it also has beta blocking activity. 02:48 I showed you in the last slide about the pulmonary fibrosis and the microcrystalline deposits. 02:55 Let's talk about the eye. Cornea verticillata. So you can see here that with the slit lamp, and you shine it on the eye, you can see these very fine, very light, very hard to see discolouration and clouding of the cornea. 03:12 You can only see it on slit lamp, but it's actually quite hard to see with a standard ophthalmoscope. 03:17 This is a classical picture of ocular changes due to amiodarone.
About the Lecture
The lecture Group 3: Potassium Channel Blockers – Antiarrhythmic Drugs by Pravin Shukle, MD is from the course Cardiovascular Pharmacology.
Included Quiz Questions
Which chiral mixture is a group 3 antiarrhythmic agent?
- Sotalol
- Propranolol
- Timolol
- Esmolol
- Atenolol
Which statement regarding group 3 anti-arrhythmic medications is most accurate?
- They block potassium channels.
- They shorten the action potential.
- They shorten the PR interval on the ECG.
- They shorten the effective refractory period.
- They increase the ventricular response to atrial dysrhythmias.
Which medications are class 3 anti-arrhythmics?
- Amiodarone, sotalol
- Amiodarone, esmolol
- Flecainide, esmolol
- Flecainide, sotalol
- Procainamide, flecainide
What is a toxicity associated with amiodarone?
- Pulmonary fibrosis
- Xerostomia
- Dry eyes
- Tinnitus
- Wet desquamation
Which medication has potential toxicities including chronic interstitial pneumonitis, thyroid dysfunction, and sinus bradycardia?
- Amiodarone
- Sotalol
- Esmolol
- Flecainide
- Procainamide
What is NOT a potential toxicity of amiodarone?
- Serositis
- Corneal verticillata
- Pulmonary fibrosis
- Prolonged QT
- Thyroid dysfunction
Author of lecture Group 3: Potassium Channel Blockers – Antiarrhythmic Drugs

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
