Playlist
Show Playlist
Hide Playlist
Arnold-Chiari Malformations and Craniosynostosis

-
Slides ICPandHydrocephalus Pediatrics.pdf
-
Download Lecture Overview
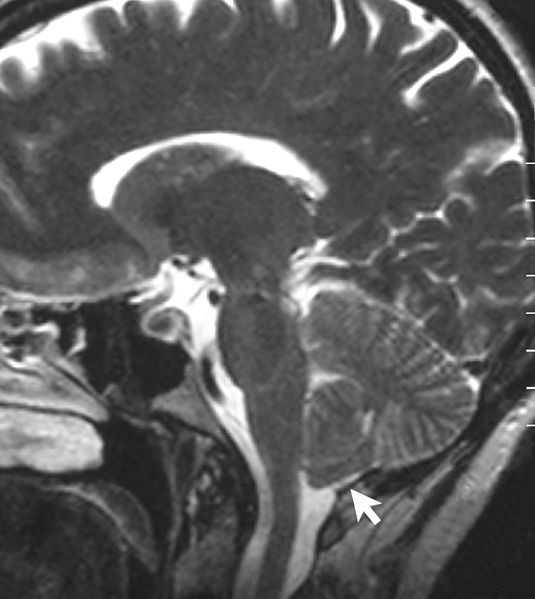
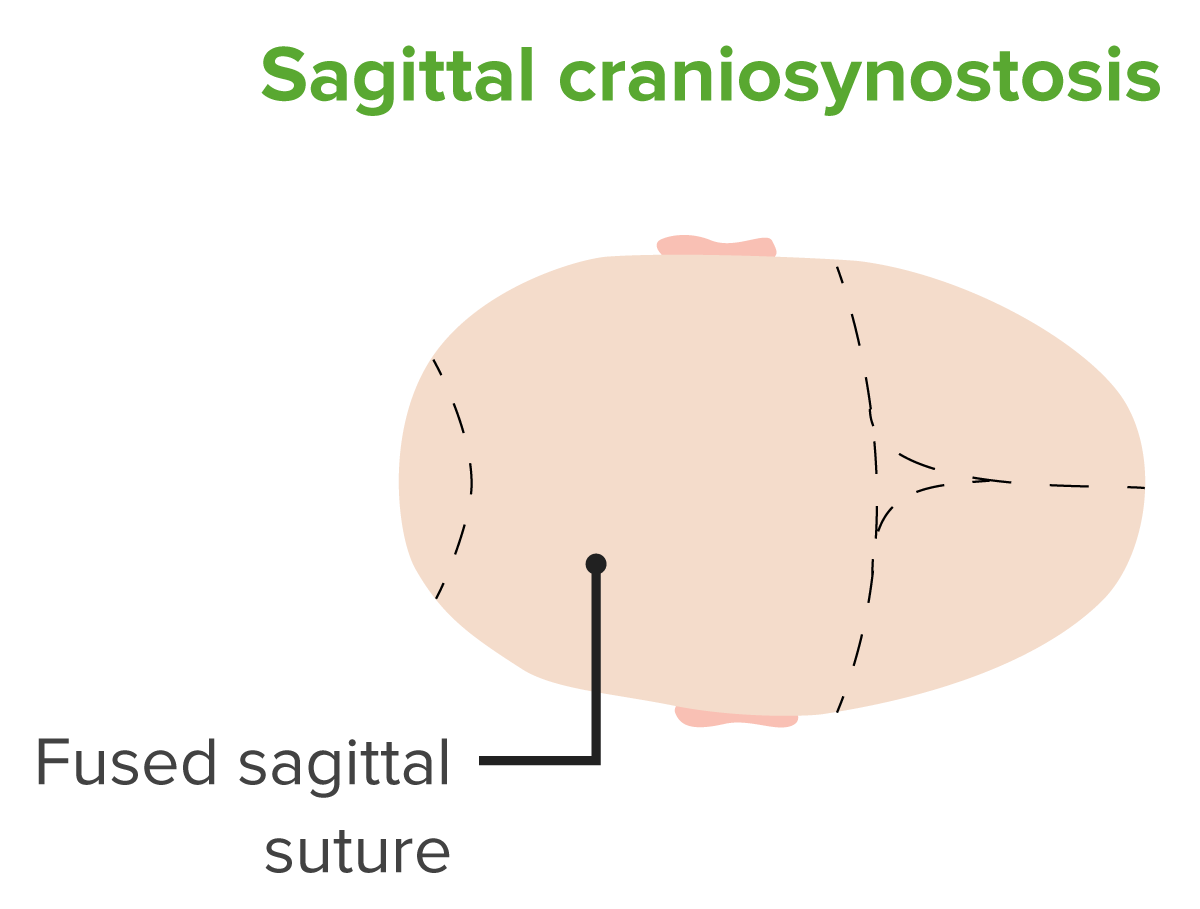
00:01 Let's switch gears now and talk about Arnold-Chiari malformations, which are a little bit farther down. 00:07 The Arnold-Chiari Malformation is a congenital CNS anomaly which is a displacement of cerebelar structures lower than that actually proceeds through the foramen magnum. 00:21 There are three types of Arnol-Chiari malformations. 00:24 One, two and three and this have worsening severity in terms of the amount of tissue this downward displaced through the foramen magnum. 00:33 Type I is generally mild and may in fact be asymptomatic and discovered in adulthood through imaging or found on an autopsy much later in life when a patient dies for some other reason. 00:47 The treatment of Arnold-Chiara Malformations if needed is generally neurosurgery. 00:54 The idea being that we want to try and prevent both the flow of CSF through these lesions but also any damage to normal tissue. 01:04 Next, let's focus on cranisynostosis. 01:08 Craniosynostosis is not a problem with the brain contents it is a problem with the skull. 01:14 Recall that in newborns, newborns are born with multiple skull pieces gradually seal together over time. 01:24 They are born for example, a frontal fontanel and a posterior fontanel and these are areas where the skull has not fused together and actually palpating the child's brain through the skin. 01:38 In the brain, there are some normal sutures that you can see in children. 01:42 There is a sagittal suture, as you can see that runs from front to back. 01:46 There is a the coronal suture, which runs left to right across the front of the brain. 01:52 And there's the lambdoid suture which is in a lambda shape which runs diagonally backwards towards the occiput from the top sagittal suture. 02:03 These are the normal skull sutures. 02:06 But children can have problems with their sutures when they prematurely fuse. 02:12 So craniosynostosis is a premature fusing of skull sutures, which prevents the skull from growing and that can cause substantial problems for the brain which is trying to grow inside and is now limited in terms of its ability to grow. 02:29 They may have localized areas of fusion such as an isolated sagittal suture, an isolated coronal suture, or an isolated lambdoid suture that have sealed shot prematurely. 02:42 Or they may have generalized disease when they have multiple suture involvement. 02:48 This results to microcephaly. 02:50 Remember, we're tracking this children's head circumference throughout their childhood and this is another reason to do it. 02:56 If we see the head circumference gradually tailing off and failing to grow, we may well suspect a generalized craniosynostosis. 03:07 These children are going to have problems with their brain development and will develop developmental delay. 03:14 They may even lose milestones if it gets very severe. 03:19 Also, patients may have syndromes. There are several general syndromes that are associated with craniosynostosis I'll give you a couple of examples. 03:30 In Apert Syndrome, patients can have Sydactyly when their fingers are fused together. 03:35 They also develop craniosynostosis. 03:39 Likewise in Crouzon Syndrome, patients may have Exopthalmos or eyes bulging outward out of their face and an associated craniosynostosis. 03:51 When we see a patient with craniosynostosis, we would often see abnormal moulding of the head. 03:58 But everytime you see a child with an abnormal head, it does not mean they have craniosynostosis. 04:06 This is a very common problem that can be mistaken for craniosynostosis. 04:12 This is plagiocephaly, which is positional mouldling. 04:16 This may happen because parents are laying their child preferentially on one side or a child may have an underlying problem. 04:25 For example, they may have an inability to move their neck from a congenital torticollis. 04:31 Thus, because they are not able to move their necks so well, they often get a plagiocephaly. 04:38 This is managed very simply, though allowing the child to move their head in different directions. 04:44 And encouraging the parents to help that child move their head in different directions. 04:48 In very severe cases, we can fit them with helmets. 04:51 But in most cases, simple physical therapy can largely correct the problem and it gradually resolves or improve as they get older. 05:02 This is sagittal craniosynostosis. 05:05 You can see that sagittal suture has been fused between the coronal suture and the lambdoid suture. 05:13 This is causing the child to have a very long and narrow head. 05:19 This is Lambdoidal craniosynostosis. 05:22 Here you can see in the posterior aspect of this child's head on his or her right side, a closed lambdoid suture. 05:31 This is causing because of angulation, a frontal protuberance and you can see the affected side has a posteriorly displaced ear. 05:42 This is a classic head configuration for a child with lambdoidal synostosis. 05:49 To make a diagnosis, we'd form a CT scan of the head. 05:52 It's necessary to do a CT scan as opposed to an MRI because CT scans are much better at seeing bone. 06:00 Remember, CT scans bone and blood. 06:03 So for this purpose, we usually get CT scans and we can do three dimensional reconstructions from the digital images to show to the surgeons; to help them decide how they can best repair this child. 06:17 Surgical repair is the mainstay of therapy. 06:20 We have to fix these skulls, so that we can expand them and allow room for the brain to grow inside. 06:27 This surgery is a major surgery. 06:30 It is bloody and it is difficult and it usually requires a multidisciplinary team of both surgeons and neurologists. 06:39 Patients and families and the doctors and nurses who care for these patients all have to work together because this is a complex and painful care. 06:49 Remember that craniosynostosis is present in several genetic syndromes. 06:54 It is important to consult a geneticist for patients who have craniosynostosis to verify that there is not an underlying genetic condition. 07:03 Genetic conditions are important to understand because it may relate to future prognosis. 07:08 And it may help the parents decide about future children and what the risk and benefits there are. 07:15 That's the brief summary of the structural problems in the heads of children. 07:19 Thanks for your attention.
About the Lecture
The lecture Arnold-Chiari Malformations and Craniosynostosis by Brian Alverson, MD is from the course Pediatric Neurology. It contains the following chapters:
- Arnold-Chiari Malformations
- Craniosynostosis
- Diagnosis of Craniosynostosis
Included Quiz Questions
An infant with torticollis since birth presents with flattening of one side of her occiput. Which of the following is the most likely diagnosis?
- Plagiocephaly
- Crouzon syndrome
- Apert syndrome
- Sagittal craniosynostosis
- Lambdoid craniosynostosis
Microcephaly is an example of which type of craniosynostosis?
- Generalized
- Localized
- Generalized with syndrome
- Multiple
- It is not a craniosynostosis
Which type of craniosynostosis displaces one ear posteriorly?
- Lambdoidal craniosynostosis
- Sagittal craniosynostosis
- Coronal craniosynostosis
- Apert syndrome
- Crouzon syndrome
Author of lecture Arnold-Chiari Malformations and Craniosynostosis

Brian Alverson, MD
Customer reviews
4,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
The explanation for craniosynostosis was very good. I wish there was more information on Arnold Chiari Malformation.
Excellent lecture, very interesting to see all these different diseases that don't get so much attention. Thanks!
