Playlist
Show Playlist
Hide Playlist
Cerebral Aneurysm: Treatment


-
Slides 03 CerebralAneurysms Neuropathology I.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
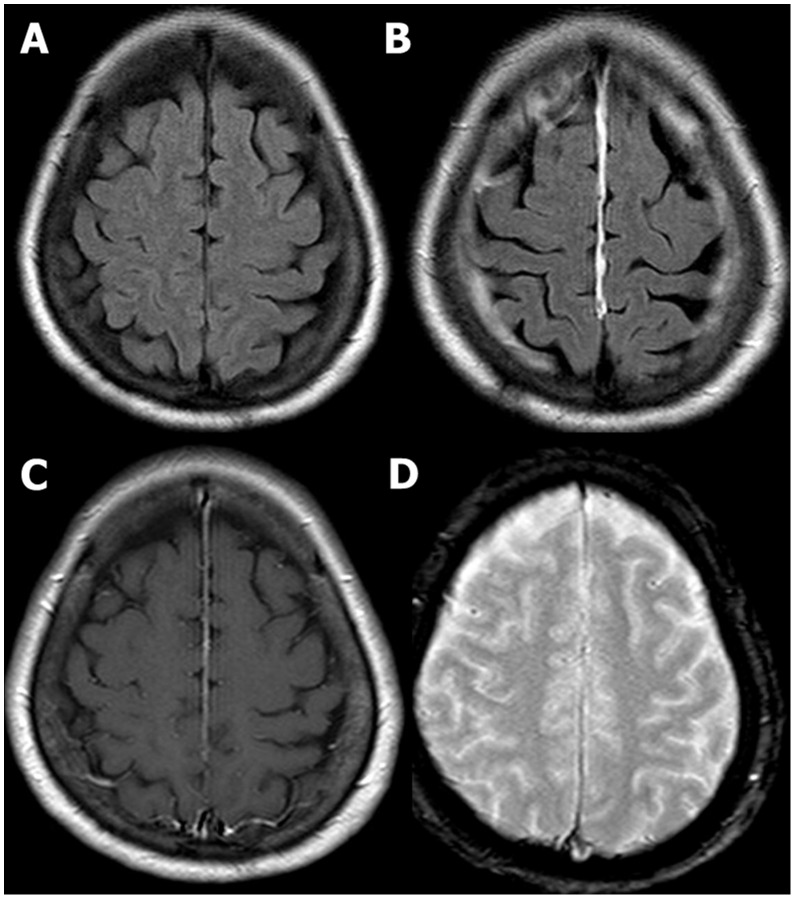
00:00 Management: Clip or coil once they identified the aneurysm, hydrocephalus is a possibility and by this you're going to then drain out the fluid intraventricular catheter. However, as soon as that happens you're always worried about what please? Infections. Vasospasms occur in 30% of patients usually 4-14 days after symptom onset and up to 21 days later. Vasospasms can cause cerebral ischemia and contribute significantly to the morbidity and mortality of a person with a subarachnoid hemorrhage. They appear to be related to the release of spasmogenic substances from lysed blood. To prevent and treat vasospasms, give nimodipine which is a calcium channel blocker, but also offers neuroprotective effects by some other unknown mechanisms. Hypertension is induced with vasopressors to maintain cerebral perfusion and euvolemia is maintained with crystalloids or colloids. An external ventricular drainage catheter is placed if there is elevated intracranial pressure or if the ventricle is enlarged indicating hydrocephalus. Continuing our discussion of subarachnoid hemorrhage, let's officially enter the topic itself. We just came off our discussion of aneurysms and if that aneurysm is to then get large enough, it ruptures in this case with the berry aneurysm that we referred to. You are then going to bleed into your subarachnoid space and perhaps even then bleed on to your intraparenchymal type of hemorrhage. The complications here, as you know, would be the worst headache that he/she has experienced called "thunderclap headache," meningismus type of symptoms, and altered mental status. On CT, you can then expect to see the type of hemorrhage that you see here. The complications that you're worried about as we had mentioned earlier, if you peak approximately 3 weeks or 21 days into your subarachnoid hemorrhage, you want to try to manage your vasospasms and there we refer to our calcium channel blocker nimodipine or you are now also having issues with properly draining your cerebrospinal fluid resulting in hydrocephalus and then increase intracranial pressure could be then managed with drainage maybe perhaps with intraventricular type of catheter. Summary. Risk factors: Age, female gender, African American race, most likely due to hypertension, smoking, stimulants, alcohol. Preventive medicine: Remember, if your patient you know is predisposed to developing an aneurysm, usually that's a 5th decade of life. Management of unruptured aneurysm, 1% of general population, any risk of SAH, is 1-2% is related to aneurysm size. Risk factors for rupture of unruptured cerebral aneurysms are namely larger size, location and the posterior circulation, and history of previous SAH. 03:13 Signs and symptoms: We talked about the headache, it could be loss of consciousness. Think of it as being like a space occupying lesion. Differential diagnoses: At some point, we have discussed cluster headaches, migraines, and meningitis are all differential diagnoses when you're dealing with subarachnoid hemorrhage. Acute and post acute diagnostic work-up: CT scan, we did a lumbar puncture, we discussed the tubes that you would find, for example, because you're continuously introducing blood into subarachnoid space. No matter how many samples you take, for RBC count it will always be pretty much elevated between 1 and 4. 03:56 Angiogram, you want to check out what cause the subarachnoid hemorrhage. And transcranial Dopplers as well could help you. In other words, ultrasound. The management here will be clipping and if we talk about coiling of aneurysm. For the prevention and treatment of vasospasm, administer nimodipine, induce hypertension with vasopressors to maintain cerebral perfusion and maintain euvolemia with crystalloids or colloids. If the intracranial pressure becomes elevated or if there is evidence of hydrocephalus as indicated by enlarged ventricles, then an external ventricular drainage catheter must be inserted.
About the Lecture
The lecture Cerebral Aneurysm: Treatment by Carlo Raj, MD is from the course Cerebral Aneurysm (Intracranial Aneurysm). It contains the following chapters:
- Cerebral Aneurysms: Treatment
- Subarachnoid Hemorrhage
- Subarachnoid Hemorrhage: Summary
Included Quiz Questions
Which of the following is part of a treatment protocol in the management of vasospasm arising from subarachnoid hemorrhage?
- Calcium channel blockers
- Aspirin
- Beta-blockers
- Opioids
- Furosemide
What is one of the possible treatments for a subarachnoid hemorrhage?
- Clip or coil placement at the aneurysm site
- Shunt to bypass the bleeding site
- tPA
- Transfusion of RBCs
- Aspirin
Author of lecture Cerebral Aneurysm: Treatment

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
