Playlist
Show Playlist
Hide Playlist
Cerebral Aneurysm: Diagnostic Workup


-
Slides 03 CerebralAneurysms Neuropathology I.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
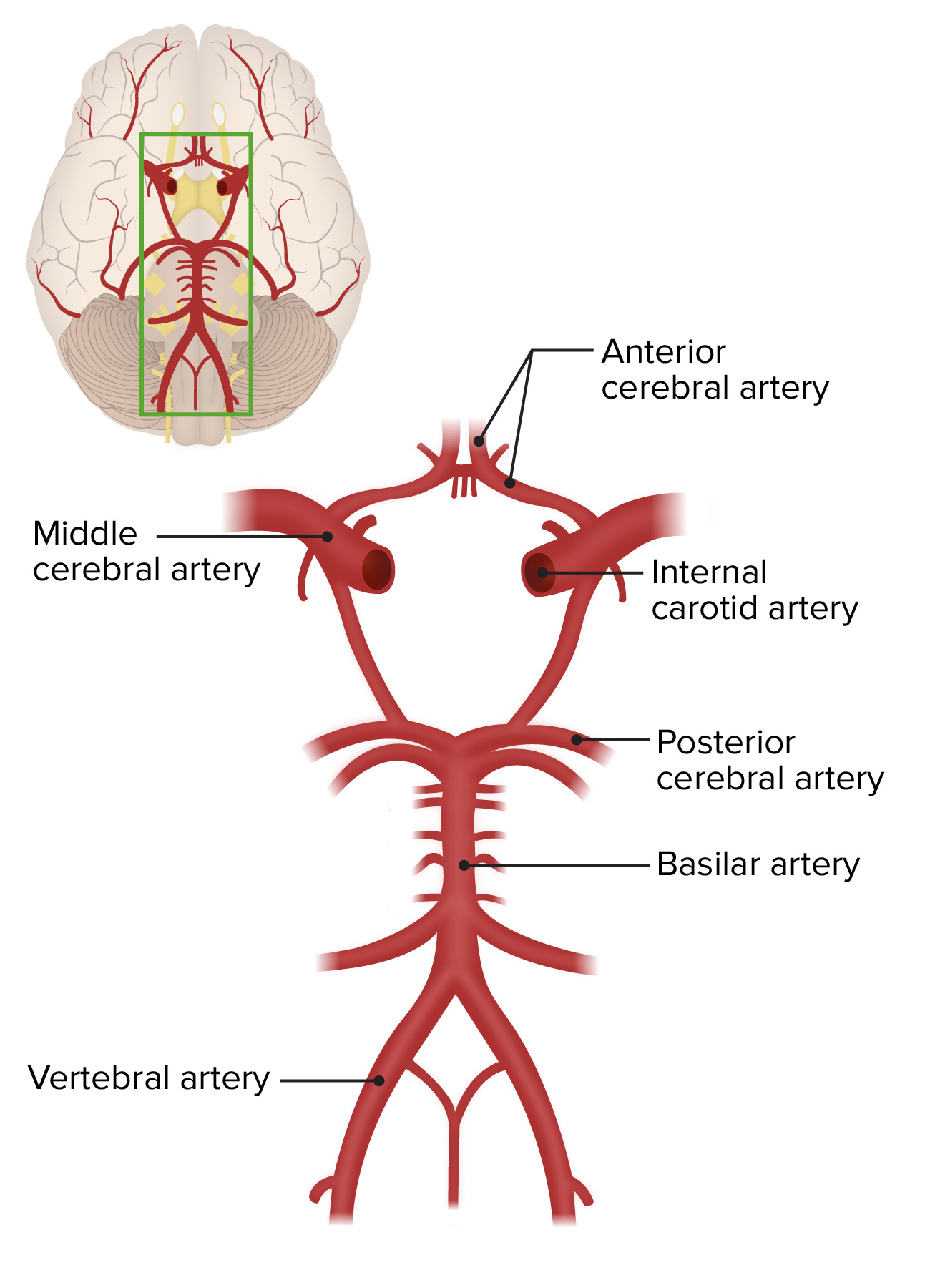
00:01 Now, those individuals that you suspect or possibly predisposing factors such as Ehlers-Danlos, Marfan, hypertension, always keep in mind, well, what’s going on with my anterior portion of the circle of Willis? Patients suspected of having SAH should have of course a non-contrast CT of the head. 00:21 4% of CT scans are unfortunately negative. 00:26 And if the CT scan is negative, then you get into a lumbar puncture. 00:31 Now, before I move on, there’s a topic that we did earlier when we looked at meningitis and then encephalitis, and I very clearly delineated the clinical differences between the two. 00:42 We spent extensive time on lumbar puncture and what you can expect in your different findings in your CSF. 00:50 Now, let me ask you a question. 00:52 And I have subarachnoid hemorrhage, and you know for a fact that the cerebrospinal fluid actually circulates where? Of course, subarachnoid space. 01:01 So now, say that there’s actual hemorrhage there. 01:04 No matter how many samplings that you would take because what you’re going to measure for here obviously is going to be what? Is it glucose? Not the obvious one. 01:15 Is it protein? Not the obvious one. 01:18 Is it hemorrhage, please? So what’s the obvious count that you’re going to look for? RBCs, right? Are we clear? This is hemorrhage. 01:25 So use common sense in terms of your clinical judgement and suspicion. 01:31 Now if there’s constant bleeding taking place into, into, the subarachnoid space, I don’t care how many samples you’ve taken. 01:38 One through four, you’re going to find RBC counts to be high from the first to the fourth compared to when it’s something like trauma in which if there’s trauma, there’s every possibility that the RBC count might start dropping. 01:50 But subarachnoid hemorrhage, not the case. 01:54 You’ll continue having high RBC count. 01:58 Patients with positive CT scan or lumbar puncture should have an angiogram. 02:03 You need to check out and confirm what exactly is causing this subarachnoid hemorrhage. 02:08 This is an important, important topic of management of your patient. 02:15 There’s something called a Hunt and Hess scale. 02:18 Asymptomatic or mild headache Moderate to severe headache, nuchal rigidity. 02:22 As we go through this, you’ll notice that when we finally get to scale of five, patient comatose. 02:30 Please know at this point as a general concept that the Hunt and Hess scale will be something that you would expect to then scale understanding as to how bad is my actual, actual headache and hemorrhage and such. 02:47 It is recommended to use the World Federation of Neurological Surgeons Scale and the Fisher Grade. 02:53 The later is based on the grading of CT findings in subarachnoid hemorrhage. 02:58 Nowadays, these are the two scales neurosurgeons use to guide their management.
About the Lecture
The lecture Cerebral Aneurysm: Diagnostic Workup by Carlo Raj, MD is from the course Cerebral Aneurysm (Intracranial Aneurysm). It contains the following chapters:
- Cerebral Aneurysms: Management of Patient
- Hunt and Hess Scale
Included Quiz Questions
What is the most likely finding in the CSF on lumbar puncture in a patient with subarachnoid hemorrhage?
- High RBC count
- High glucose
- High protein
- High WBC count
- Elevated opening pressure
A patient suspected of having a subarachnoid hemorrhage should have which test first?
- Non-contrast CT
- Lumbar puncture
- ECG
- MRI of the brain
- Contrast CT
Author of lecture Cerebral Aneurysm: Diagnostic Workup

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
