Playlist
Show Playlist
Hide Playlist
Case: 74-year-old with Cognitive Dysfunction

-
Slides Alzheimer Dementia.pdf
-
Download Lecture Overview
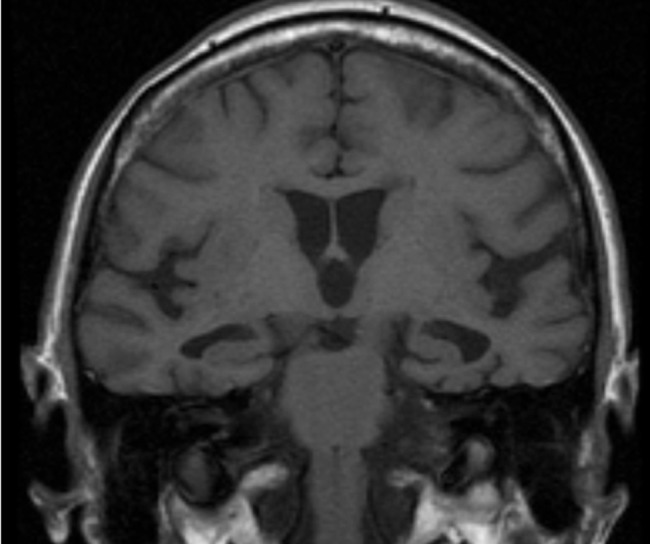
00:00 Now, let's turn to a case. This is a 74-year-old who presents with cognitive dysfunction. 00:07 The patient and family reports 3-5 years of progressive memory loss and executive dysfunction. This first began about 5 years ago when the patient began to have difficulty with remembering new things like dates, names. Would forget keys, directions, and have difficulty with driving. Over the past few years, the patient has increasingly withdrawn from friends and other social activities as memory loss has progressed. The patient no longer assists with finances and over the past year there has been a concern with cooking and baking and safety around the home. 00:41 And so these tasks are now done primarily by the patient's family. On exam, the patient is alert, awake, oriented to location and to being in the hospital clinic. 00:54 The patient had significant memory impairment, registering 3/3 items with immediate recall so there we asked the patient to remember 3 items and asked them immediately and this patient is able to register those items, but is only able to recall 1/3 at 5 minutes. So this is a problem with short-term memory. The patient is able to name objects and is fluent and follows commands. There is no aphasia. 01:19 The patient has reduced attention and concentration, frontal lobe tasks that are impaired, and is unable to report the months of the year backwards. There is reduced overall fund of knowledge. There are no other remarkable findings and no other focal deficits on exam. So what's the most likely diagnosis in this patient? Is his Alzheimer's disease frontotemporal dementia, Lewy body dementia, or mild cognitive impairment? Well, this is not the typical presentation of frontotemporal dementia. Frontotemporal dementia affects primarily the frontal lobes, the temporal lobes, and behavior function. We see symptoms of speech aphasia, speech dysfunction, semantic dementia and behavioral changes which are not prominent in this case. This is not the typical description of Lewy body dementia. 02:11 Patients with Lewy body dementia present with cognitive dysfunction often subcortical dysfunction as well as early Parkinsonism which we don't have on exam or by report for this patient. This is not mild cognitive impairment. The patient's cognitive dysfunction is significantly affecting their daily function. 02:29 They have retracted from social activities or no longer working and now there is a concern about cooking, baking, and safety in the home. This is a typical presentation of a patient with Alzheimer's disease.
About the Lecture
The lecture Case: 74-year-old with Cognitive Dysfunction by Roy Strowd, MD is from the course Alzheimer Dementia.
Included Quiz Questions
How might a clinician differentiate Alzheimer disease from frontotemporal dementia?
- Patients with frontotemporal dementia are more likely to display speech aphasia, speech dysfunction, and behavioral changes.
- Patients with frontotemporal dementia are more likely to display deficits in concentration and attention, along with short-term memory loss.
- Patients with Alzheimer dementia are more likely to display subcortical dysfunction as well as early parkinsonism.
- Patients with Alzheimer dementia are more likely to display speech aphasia, speech dysfunction, and behavioral changes.
How might a clinician differentiate Alzheimer disease from dementia with Lewy bodies?
- Patients with dementia with Lewy bodies are more likely to display subcortical dysfunction as well as early parkinsonism.
- Patients with Alzheimer dementia are more likely to display subcortical dysfunction as well as early parkinsonism.
- Patients with Alzheimer dementia are more likely to display global aphasia and hallucinations early in the disease course.
- Patients with dementia with Lewy bodies are more likely to develop deficits in concentration and attention, along with short-term memory loss.
What are some of the classic symptoms associated with Alzheimer dementia?
- Deficits in concentration and attention, along with short-term memory loss
- Progressive mutism and choreiform movements late in the disease course
- Bradykinesia, rigidity, and a resting tremor
- Urinary incontinence, a "magnetic" ataxic gait, and behavioral changes
Author of lecture Case: 74-year-old with Cognitive Dysfunction

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
