Playlist
Show Playlist
Hide Playlist
Case: 58-year-old Woman with Headache

-
Slides Other CNS Infections.pdf
-
Download Lecture Overview
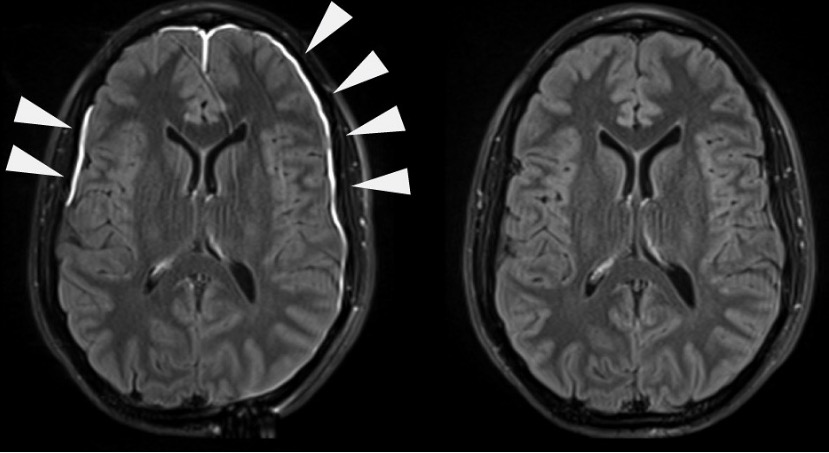
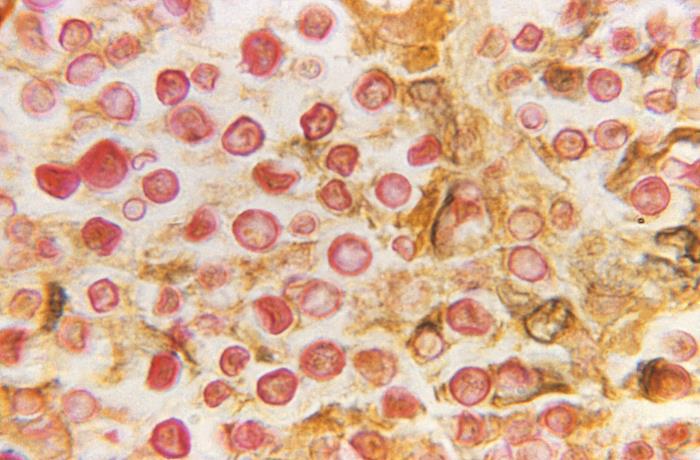
00:00 In this lecture, we're going to talk about other types of CNS infections and in particular opportunistic and exposure-related CNS infections. So let's start with a case. A 58-year-old woman with headache. This is a 58-year-old Black woman with a past medical history of lupus who has been managed for over 10 years with multiple immunosuppressing agents; hydroxychloroquine, mycophenolate, and prednisone requiring prednisone doses up to 40 mg per day and we think of prednisone doses over 20 mg being immunosuppressive. She presents with a 1.5-week history of headache, confusion, and episodes of strange stereotypic spells that could be seizures. And lo and behold this culminated in a generalized tonic clonic seizure for which she was admitted to the hospital. Examination shows that she is confused, but is conversant. She has no focal neurologic deficits. And CSF analysis is performed showing increased white blood cells (pleocytosis), elevated proteins, secondary inflammation, and low glucose suggesting that if this is an infection, this is a fungal process. The CSF is also tested for the cryptococcal antigen, evidence of a cryptococcal infection and is elevated with a titer of 1 and 64. So what's the diagnosis? Well, there are some really important features of this case that we should key in on. The first is this is a patient who is immunocompromised. She has been on multiple immunosuppressing medicines for over 10 years which could affect her immune system's ability to prevent those atypical or rare causes of meningitis, encephalitis, and cerebritis or brain abscess. The second is there is evidence of cortical dysfunction. Not a focal deficit. Her exam does not have any focal deficits, but a generalized brain process with this generalized tonic clonic seizure suggesting an encephalitis or meningoencephalitis. And the last is the CSF analysis and this is a classic signature for a fungal encephalitis and even more important we see evidence of cryptococcal antigen positivity suggesting a possible cryptococcal infection. The patient had imaging to further evaluate what may be going on and here we're looking at the axial on the left and the coronal post contrast T1 gadolinium enhanced images. And what we see is very subtle. The brain in general looks normal, but in the folia of the cerebellum, those potential spaces in between the gyri of the cerebellum in the sulci, we see enhancement, extra white, extra gadolinium contrast there indicating that something is in the spinal fluid. And here, this is evidence of a cryptococcal infection and suggestive of a cryptococcal meningoencephalitis. So what is the diagnosis? Is this cryptococcus, toxoplasmosis, neurocysticercosis, or a brain abscess? And as we've discussed, toxoplasmosis has a predilection for the basal ganglia. This doesn't seem like toxoplasmosis. Neurocysticercosis can be seen in immunocompromised patients but is more common in patients who have travelled to areas where neurocysticercosis is endemic and we don't get that history here. We don't see evidence of a brain abscess, there is not a focal finding on exam and the evidence on imaging doesn't suggest a focal brain infection. And so this is a classic presentation of cryptococcal meningitis or cryptococcal meningoencephalitis. The CSF analysis suggests a fungal infection and the positive cryptococcal antigen establishes the diagnosis. So in this lecture, we're going to talk about 3 types of opportunistic or exposure-related CNS infections. There are many, more than just the 3 we'll discuss but these 3 are particularly common, we see them in patients or tested in clinical vignettes. So I'd like you to understand how to apply what we learn with each of these 3 organisms to any opportunistic or exposure related infection in the brain. As you can see here, there are a variety of these opportunistic infections that if primarily been described in AIDS patients, but increasingly we see them in patients on immunocompromising or immuno-active medications. We also need to think about exposure associated infections. 04:35 Infections that occur in certain types of the world and certain areas over the country and in patients who have travelled to those areas. Today, we're going to talk about cryptococcus, toxoplasmosis, and neurocysticercosis.
About the Lecture
The lecture Case: 58-year-old Woman with Headache by Roy Strowd, MD is from the course CNS Infections.
Included Quiz Questions
Which of the following CNS infections has a predilection for the basal ganglia?
- Neurotoxoplasmosis
- Neurocysticercosis
- Herpes encephalitis
- Cryptococcal meningoencephalitis
- Gonococcal meningitis
Which of the following CSF findings is suggestive of a fungal infection?
- High protein
- Normal glucose
- Many red blood cells, some showing lysis
- Low cell count
- Low opening pressure
The diagnosis of cryptococcal meningoencephalitis can be established with ...?
- ...a CSF cryptococcal antigen assay.
- ...blood, sputum, and urine cultures.
- ...a T1-weighted gadolinium-enhanced MRI.
- ...a complete metabolic panel.
- ...a complete blood count.
Author of lecture Case: 58-year-old Woman with Headache

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
