Playlist
Show Playlist
Hide Playlist
Cardiac Case: 24-year-old Man with Asymptomatic Murmur

-
Cardiac Case 24-year-old Man with Asymptomatic Murmur.pdf
-
Reference List Cardiology.pdf
-
Download Lecture Overview
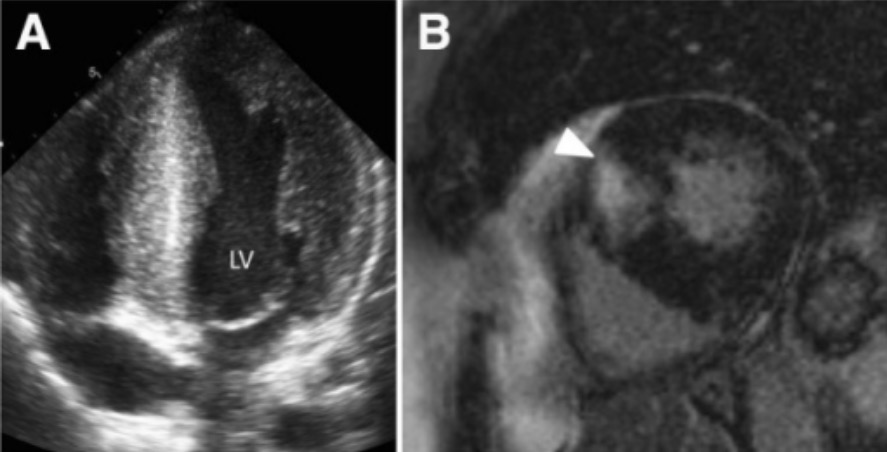
00:01 A 24-year-old weight lifter is referred to you for evaluation of a murmur. 00:05 Patient has no symptoms, he says, 'I'm super healthy', he's an amateur competitive weight-lifter, trains nearly every day lifting more than 200 pounds multiple times during each session. 00:17 On physical exam, blood pressure's normal, everything's normal except that there's an abnormality in his heart findings. 00:24 His heart sound shows a prominent S4, a grade 3/6 systolic ejection murmur heard all over the precordium, and an increase in loudness with Valsalva maneuvers and diminishes with squatting. 00:37 So, let's hear that. First of all, the S4. Here's normal, lub-dub, lub-dub. 00:43 Here's the fourth heart sound, vlub-dub, vlub-dub, vlub-dub. 00:48 You hear a little sound just before the first heart sound. 00:51 And now, he's going to have a loud, harsh systolic ejection murmur, vlub-whoo-dub, vlub-whoo-dub, vlub-whoo-dub So, you can hear a very loud murmur when he of course does Valsalva maneuver, the murmur gets louder. So, it goes from whoo, whoo, whoo, whoo, whoo, whoo, and if he squats it gets softer. 01:14 These findings are very suggestive of hypertrophic cardiomyopathy with subaortic obstruction. 01:21 The rest of the physical exam is normal and all of his blood tests are normal. 01:25 And again, critical in here in the physical exam is a suggestion of hypertrophic obstructive cardiomyopathy. 01:32 He has an echocardiogram which shows marked hypertrophy of the left ventricle and the left ventricular wall is markedly thickened but fortunately he doesn't have a gradient across the left ventricular outflow tract so this is a less worrisome form of hypertrophic cardiomyopathy. 01:52 Some forms, particularly where there's a large gradient across the left ventricular outflow tract, patients are at risk for sudden death particularly with exertion and in addition, if the patient has massive hypertrophy, that also puts the patient at risk for sudden death. 02:09 And finally, their families where the history of sudden death is present and that of course increases the risk for a bad event happening. 02:17 Well, the hypertrophic cardiomyopathy is the commonest congenital heart form of disease. 02:25 It's an autosomal dominant inherited disease. It's usually benign in most patients. 02:30 Most mutations occur in the genes for the myocardial contractile apparatus. 02:36 It is associated with a small increased risk of sudden death during athletic exertion and in a few cases, there's severe mitral regurgitation and you have to replace the mitral valve because one of the papillary muscles gets pull over during contraction causing MR. 02:54 And the murmur results from some obstruction in the outflow tract and as I mentioned during systole but in this, our patient's instance, there wasn't a gradient so it's not of any main concern. 03:07 And so, just to be safe with this patient, we do a maximum exercise test which shows no arrhythmias whatsoever? We do a 24-hour Holter monitor which shows no abnormal heartbeats. 03:20 And consequently, he's had no syncope or near syncopal episodes. 03:25 We think he's probably safe to continue weight training. 03:28 We'd talk to him about possible symptoms that might be worrisome but we think it's okay for him to continue his weight training. 03:36 This is something that could be argued by different cardiologists. 03:40 Some might say he should change sports but given all of the re-encouraging signs from his various examinations, I think it's safe for him to continue to weight lift. 03:51 This is the number one cause of death in athletes in the US and as I said, it usually occurs in people that have a big gradient across the outflow tract or people where there's a family history of hypertrophic myopathy with sudden death.
About the Lecture
The lecture Cardiac Case: 24-year-old Man with Asymptomatic Murmur by Joseph Alpert, MD is from the course Cardiovascular Cases.
Included Quiz Questions
A 24-year-old weightlifter presents for evaluation of a murmur. He has no symptoms. He is an amateur competitive weightlifter and trains nearly every day, lifting more than 200 pounds multiple times during each season. During cardiac auscultation, a prominent S4 and a grade 3/6 systolic ejection murmur are detected. The rest of his physical examination findings are normal. The patient's blood test results are normal. An echocardiogram is performed, and marked thickening of the left ventricular walls without evidence of gradient across the left ventricular outflow tract is detected. Which of the following is TRUE regarding this patient's heart murmur?
- The murmur will get softer with squatting.
- The murmur will get softer with the Valsalva maneuver.
- The murmur will get louder with squatting.
- The murmur will get softer upon abrupt standing
- There will be no changes in murmur intensity with the Valsalva maneuver.
Author of lecture Cardiac Case: 24-year-old Man with Asymptomatic Murmur

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
