Playlist
Show Playlist
Hide Playlist
Bronchiectasis: Cystic Fibrosis

-
Slides ObstructiveLungDisease Bronchiectasis RespiratoryPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
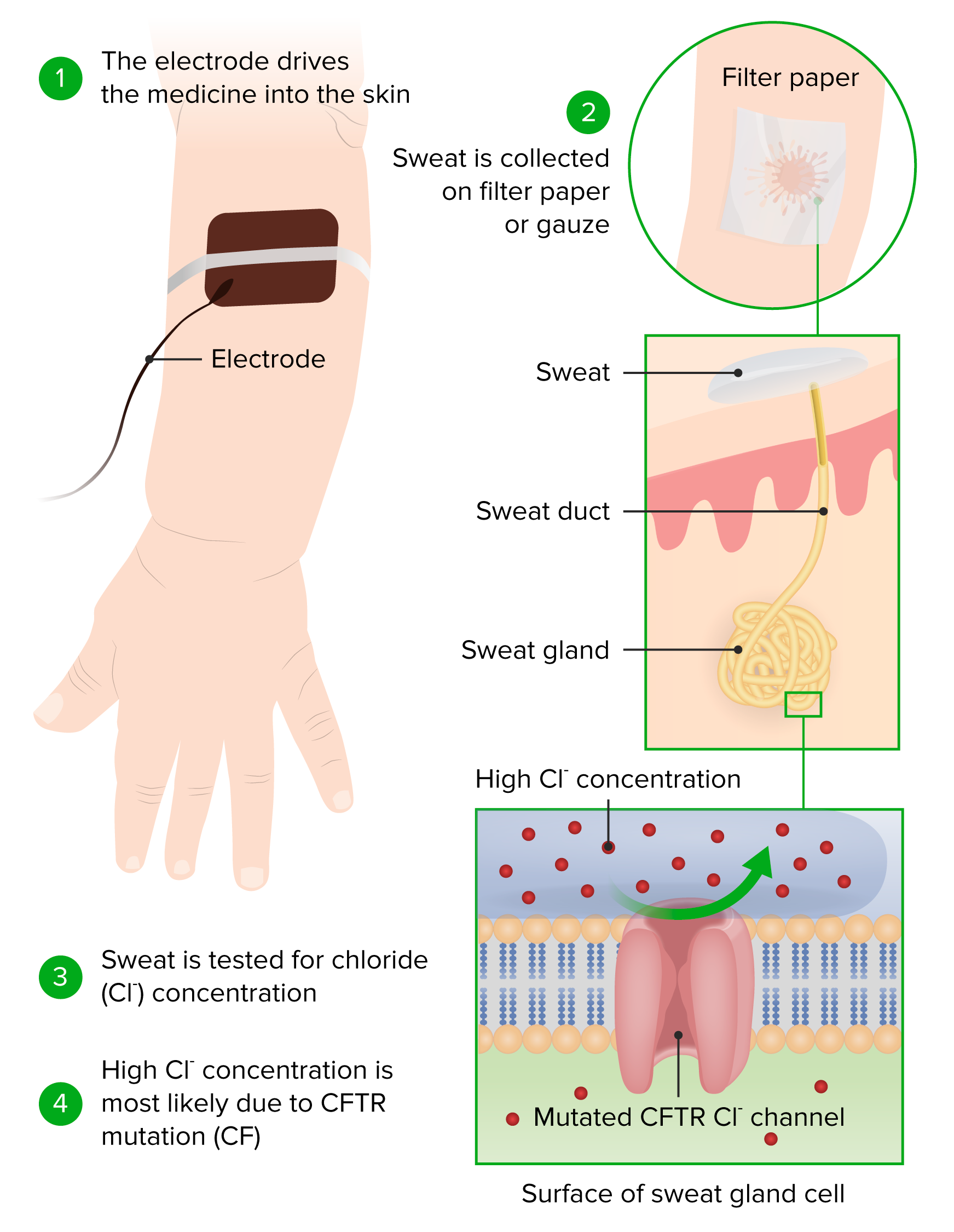
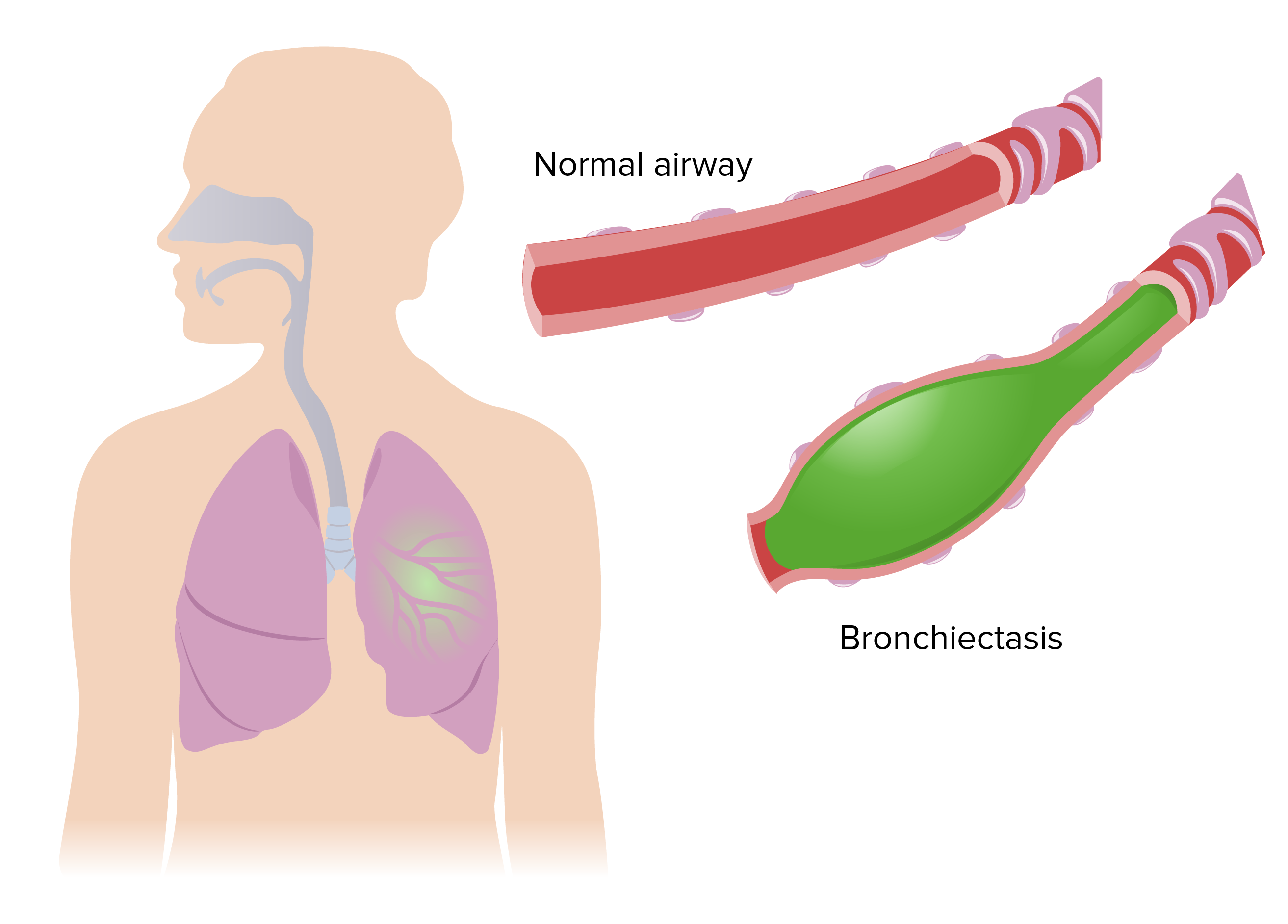
00:02 Here we have one of the three most lethal genetic diseases in the caucasian population in the US Welcome to Cystic Fibrosis. 00:12 The other two being alpha-1 antitrypsin deficiency and Down's Syndrome. 00:17 In cystic fibrosis remember, it is inherited, autosomal recessive mutation being in the cystic fibrosis transmembrane regulatory protein or gene which is a chloride channel. 00:30 Remember, the chromosome by chance form biochemistry or genetics? Good, chromosome 7. In the specific was Phe508. 00:41 That at least you must know. 00:43 Now before I move on, we'll predict as to what we can find in our patient, just like we would do any case, draw up a prediction, right? So normally speaking, remind me if it's in sweat. 00:56 That CFTR or chloride channel, does it absorb or does it secrete? It normally is going to absorb, isn't it? Let's talk about that one first. 01:06 So normally, if that channel is to absorb and now the chloride channel is dysfunctional Now you taste your infant... no I'm joking don't do that, that's kinda creepy, but you're definitely going to do a sweat chloride test So therefore, you'd expect there to be an increase in chloride concentration up to as much as or greater than 60mEq per liter And that takes care of the sweat chloride test, correct? Now remind me what may then happen in your ducts. 01:36 and by ducts, referring to bronchioles and maybe the pancreatic. 01:42 When your duct.. what you end up happening, what's supposed to do in your duct is the chloride channels are supposed to secrete chloride. 01:50 What's secrete mean? It's supposed to go into the duct, right? So now that the channel's no longer working for chloride, it remains behind in your cell. 02:00 Now, chloride is an anion. 02:02 It cannot live by itself ever. 02:04 It has to maintain a neutrality, that is how our body's built Obviously chloride is an anion, its neutralizer would then have to be what, please? Sodium. 02:14 So now sodium hurriedly comes out of the duct and comes into the cell to then accompany that lonely chloride. 02:22 And there you have it, sodium comes in but sodium doesn't also come in by itself, does it? along with it would be water as well. 02:29 Now let us read this statement. 02:31 Suspect a newborn child with hyponatremic dehydration, unless sodium is leaving But the sweat chloride test would be high. 02:41 failure to thrive, of course. 02:43 or an adult with sinus disease, and why would there be bronchiectasis? Remember, you'd have bronchiectasis in your lungs because the secretions or the viscosity in your duct is very very thick now You may then resut in chronic bronchitis and eventually may result in bronchiectasis. 03:03 In addition, the same type of issue or in a male especially may result in infertility Whereas in a female, it might be subfertility in which the lady would have amenorrhea for example Now that we took care of the lungs, let's take a look at the pancreatic duct Now please picture the pancreatic duct for me please Coming out of the head, and you're moving towards your second part of duodenum, correct? to the ampulla of vater. 03:30 or now the duct becomes extremely thick and viscous, things are gonna back up and you're gonna end up developing acute pancreatitis in perhaps a child How would you know? Well the child is now grasping to the stomach and maybe perhaps grasping to the back, right, because of radiation to the back. 03:47 Now that you lose pancreatic function in this child, you're gonna result to malabsorption, aren't you? And by malabsorption, referring to the fact that well, I'm gonna have statorrhea because I can't take in my fat. 04:00 If I can't take in my fat then I'll also lose the ability to absorb fat-soluble vitamins ADEK - (Vitamins) A, D, E, K So what would be nice in terms of management, what're you gonna do? Why not take care of the lungs? Take care of the lungs by giving, well maybe beta-2 agonism to open them up There's malabsorption so why not give pancreatic enzymes so that you can increase the absorptive rate of fat And so that you can take up the middle chain fatty acids and such So bronchiectasis is something that you wanna treat the pancreatic insufficiency is something that you wanna treat and with high fat diet in replacement enzymes. 04:40 Remember without the pancreatic enzyme, this would no longer work right? The management. This is really important for cystic fibrosis. 04:48 Next, well if you have such inflammation taking place, at some point in time, these bronchioles start getting damaged. 04:58 So obstructive diseases in which the bronchioles, the small airways start undergoing obstruction, it's what you're worried about. 05:07 Classic etiology, for example if you have a child, One of the most common causes of viral pneumonia in children in fact is RSV - Respiratory Syncytial Virus and it will be in winter months perhaps in closed quarters and daycare centers where all the children are running around and in close encounter with one another. 05:28 Not usually to hear squeaks on pulmo exam with wheezing, so you might find that quite often. 05:35 Non-infectious etiologies as well, bronchiolitis obliterans, we talked about that in conditions where you have increased fibrosis deposition The last time we looked at such a condition was dealing with chronic bronchitis in which there is increased deposition of fibrosis resulting to loss of your bronchioles Other times we will also take a look at this is going to be in issues such as what is called as hypersensitivity pneumonitis so these are going to be issues in which there's going to be a fibrotic peribronchiole type of bronchiolitis resulting in bronchiolitis obliterans. 06:13 It could also be seen with rheumatoid artritis as well immune destruction, autoimmune specifically.
About the Lecture
The lecture Bronchiectasis: Cystic Fibrosis by Carlo Raj, MD is from the course Obstructive Lung Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is necessary to treat pancreatic insufficiency in cystic fibrosis?
- High-fat diet and replacement enzymes
- High-protein diet and replacement enzymes
- High-cholesterol diet and replacement enzymes
- High-fat diet and replacement proteins
- High-carbohydrate diet and replacement enzymes
Which of the following organs is not commonly involved in cystic fibrosis?
- Heart
- Pancreas
- Gonads
- Lungs
- Salivary glands
Which of the following patients likely suffers from cystic fibrosis?
- Young patient with hyponatremic dehydration.
- Young patient with hypernatremic dehydration.
- Young patient with hypokalemia.
- Young patient with hypervolemia.
- Young patient with hyperkalemia.
Which of the following nutrients fail to get absorbed in a patient with cystic fibrosis?
- Vitamins A, D, E, and K
- Vitamins A, D, E, and C
- Vitamins A, B, E, and K
- Vitamins B1, B2, B12
- Vitamins A, D, E, and B complex
Which of the following viruses is the most common cause of bronchiolitis in children?
- Respiratory syncytial virus
- Pseudomonas aeruginosa
- Rhino virus
- Influenza virus
- Adeno virus
Which of the following is correct regarding cystic fibrosis?
- Autosomal recessive mutation in the chloride channel, on chromosome 7
- Autosomal recessive mutation in the calcium channel, on chromosome 7
- Autosomal recessive mutation in the chloride channel, on chromosome 17
- Autosomal recessive mutation in the sodium channel, on chromosome 7
- Autosomal recessive mutation in the chloride channel, on chromosome 11
Author of lecture Bronchiectasis: Cystic Fibrosis

Carlo Raj, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I love his lectures. He seems to make it stick.
The content is OK, but Dr. Raj speaks really fast sometimes and makes it difficult to follow him.
