Playlist
Show Playlist
Hide Playlist
Breast Cancer Classification

-
Slides Breast Female Repro.pdf
-
Download Lecture Overview
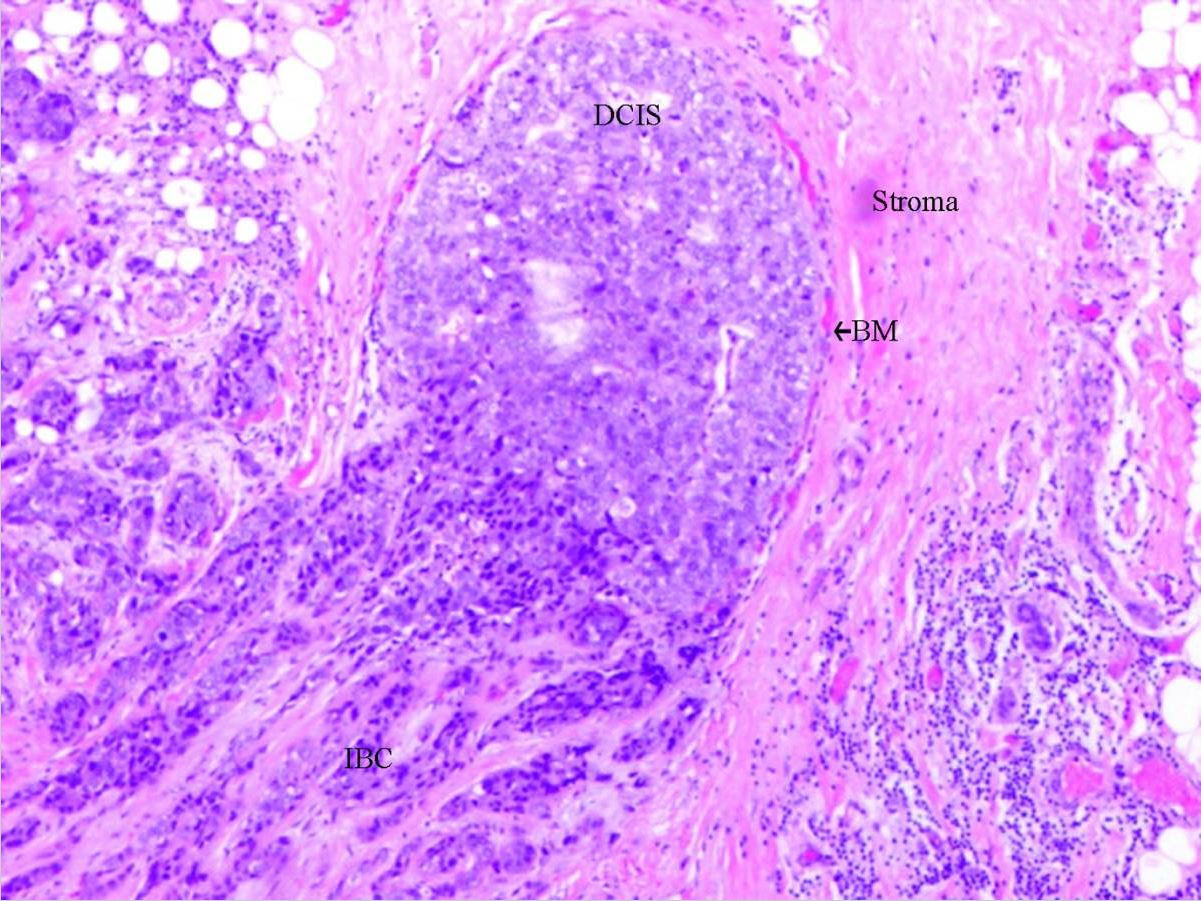
00:01 Classification: In situ, ductal and lobular. 00:05 Stop here for one second. 00:07 What does in situ mean to you? Malignancy. 00:11 What’s the difference between this and invasive? In situ, the basement membrane is intact and if it’s ductal, can you picture it? Major terminal duct and the membrane’s intact. 00:25 I’d walk you through comedocarcinoma already. 00:28 Lobular carcinoma in situ, the lobule and its membrane will be intact. 00:32 What happens now? There’s every possibility that the basement membrane is then going to rupture. 00:37 Welcome to invasive. 00:39 Would you please tell me as to what is the most common invasive breast cancer? It’s this one. 00:46 Invasive ductal cancer. 00:48 Lobular carninoma, invasive type. 00:51 Upon histology, it would show you those cells that would be all marching one behind the other. 00:59 And this is the one that loves to spread. 01:01 This is the one that loves to spread to the other breast in fact, contralateral. 01:07 Non-invasive with in situ: Malignant population of cells that lack the capacity to invade. 01:13 Acini are distorted, unfolded and take appearance of small ducts. 01:17 Non-invasive in situ. 01:20 With in situ, special subtype, we’ll walk you through comedocarcinoma. 01:23 What does that mean to you? This means that inside the actual tumor, you’d find areas that are necrotic, characterized by solid sheets of high-grade malignant cells and central necrosis. 01:34 Comedo-, comedocarcinoma. 01:37 There’s another subtype here, punctate area of necrotic material with comedone-like appearance. 01:44 The other subtype, I’m not going to spend so much time with, but you pay attention to the comedo, which to you should mean central, necrotic areas. 01:54 Now what’s interesting about this one is the following: First, take a look at the histologic picture and you find Paget cells. 02:01 The Paget cells are filled with mucin and it would stain for positive periodic acid-Schiff. 02:07 "So why in the world, Dr. Raj, are you talking about ductal carcinoma in situ and show me a picture of Paget’s? Before we begin, can you picture the patient with Paget’s disease in the nipple and how she’s presenting. 02:19 Either by picture or through description. 02:22 There’s an eczematous -- eczematous -- rash on the nipple. 02:26 Eczematous, not like skin of an orange. 02:29 And when I briefly walk you through Paget’s disease, I told you that there would have been underlying disease. 02:37 This is what I’m referring to. 02:39 Ductal carcninoma in situ, the one subtype we talked about earlier was comedocarcinoma. 02:46 Keep that separate. 02:47 Paget’s disease of the nipple which looks like eczema on the nipple. 02:50 Picture that first. 02:52 Histology shows you Paget cells. 02:55 The other time that I’ve shown you Paget cells was extramammary with vulva. 03:01 Ductal carcinoma in situ that extends from the nipple duct into the contiguous skin of the nipple and areola, the underlying cancer that you’re worried about here most of the time with Paget’s would be DCIS. 03:15 The nipple and areola are frequently fissured, ulcerated and oozing because of extreme involvement of the nipple itself. 03:24 So you want to be really careful and organize your thought here, ductal carcinoma in situ, comedocarcinoma, ductal carcinoma in situ being the underlying malignancy for Paget’s disease of the nipple. 03:36 With the duct being involved, thus you would find there to be nipple and areola that are often involved with fissures, ulcerations and oozing. 03:48 Now, let’s move on to lobular carcinoma in situ. 03:51 First, think about the lobule. 03:54 Back deep by the stroma, the lobule. 03:57 Manifested by proliferation in one or more terminal duct or ductule along with the lobule. 04:02 Here, you’d find more or less your Signet ring cells. 04:05 Stop here for one second. 04:07 Doesn’t that sound awfully familiar? Signet ring? I know that, I know that. 04:12 I know you do. 04:13 The last time we talked about this was gastric adenocarcinoma, diffuse type. 04:19 And also we talked about this in ovarian cancer. 04:23 Do you remember how you can find the Signet ring cells in an ovary or histologic picture of an ovary. 04:29 Krukenberg. 04:30 Exactly, very good. 04:31 So why is Signet-ring cell here and what kind of – "Dr. Raj, I know you’re going bring in parallel." Of course, I am. 04:39 And this is more molecular in nature. 04:42 Molecularly speaking, your diffuse type of gastric adenocarcinoma and the lobular carcinoma, they love to spread. 04:51 They’re both E-cadherin negative. 04:53 Keep that in mind, especially as we get into invasive lobular cancer. 04:58 So therefore, interesting enough, two major cancers that are E-cadherin negative contain Signet ring cells, which are filled with mucin. 05:09 Distends glandular acini. 05:12 Invasive cancer. 05:14 So what does invasive cancer mean to you? Invasive carcinoma will be one in which marked by increased and dense fibrous stroma giving a stoney hard – feel your chin. 05:26 It feels like this, gritty. 05:28 Really gritty. 05:31 Corresponds to histologic desmoplasia. 05:33 Stop here for one second. 05:35 Big time important. 05:36 Invasive pathology. 05:37 You’ve learned about a phenomenon that takes place with adenocarcinoma in which the surrounding tissues undergo a fibrous change. 05:46 Some pathologist will call it fibroplasia. 05:49 Some pathologist and on your boards, they most likely will call it desmoplasia. 05:53 So it’s a non-neoplastic but it’s fibrous. 05:56 Trying to wall off the invasion is what the response is trying to do, but in the process, it actually makes it difficult for chemotherapy to reach the cancer. 06:07 So where is their research? Guaranteed in your practice, oncology especially, that you would be giving – or you were thinking about when to give desmoplasia inhibitors. 06:20 If you remove the wall, it makes it easier to reach the cancer cell, chemotherapy. 06:24 Big time important in every way shape or form. 06:28 You may have infiltrative attachment to the surrounding structure with fixation, the dimpling of the skin, retraction of the nipple. 06:35 All of these is then known part of your invasive cancer. 06:39 Invasive lobular cancer is where we are. 06:41 These tend to be bilateral. 06:44 Remember, the most common invasive would be your? Good. 06:48 Ductal. 06:49 You definitely want to know about lobular invasive, however. 06:52 This is the one that loves to spread. 06:55 Bilateral. 06:56 Multicentric. 06:57 E-cadherin negative. 06:59 Diffusely invasive pattern. 07:01 Frequently metastasize to where? Cerebrospinal fluid, ovary, uterus, bone marrow. 07:07 All over the place. 07:09 The parallel that you want to bring here once again, remember we’re talking about Signet ring cells. 07:14 We talked about E-cadherin negative. 07:16 This one loves to spread as well. 07:18 Look at the places it loves to spread. 07:19 Everywhere. 07:21 CSF, ovary, uterus, bone marrow, so on and so forth. 07:24 This is medullary cancer. 07:26 BRCA1 is the gene here. 07:28 Soft, fleshy consistency. 07:30 Well-circumscribed is what you would expect upon morphology. 07:34 Good prognosis. 07:35 Not a whole lot to say about medullary, but you want to be familiar or know that it exists. 07:41 Poor prognostic factors, however, include high nuclear grade, aneuploidy, absence of hormone receptors, p53 expression, high proliferative rates. 07:54 So this would then make your medullary cancer to be then poor prognostically. 07:59 Our topic here very importantly is prognostic factors for breast cancer. 08:03 I’ve mentioned a few times now that the most important prognostic indicator would be axillary lymph node spread. 08:09 Tumor size will then influence your prognostication. 08:14 Estrogen and progesterone receptor expression would then help you with prognosis and if you find this to be positive, then you have drugs at your disposal such as your partial agonist, tamoxifen. 08:27 If there is increased proliferative rate, this then affects your prognosis. 08:31 And over expression or hyperexpression of HER-2/neu has worse prognosis. 08:37 However, we have a drug that we are quite familiar with, trastuzumab.
About the Lecture
The lecture Breast Cancer Classification by Carlo Raj, MD is from the course Reproductive Pathology: Breast Disease with Carlo Raj. It contains the following chapters:
- Breast Carcinoma Classification
- Differential Diagnosis of Non-Invasive Carcinoma
- Differential Diagnosis of Invasive Carcinoma
Included Quiz Questions
Which of the following statements about comedocarcinoma is INCORRECT?
- It is a type of lobular carcinoma in situ.
- It presents with solid sheets of high-grade malignant cells with central necrosis.
- Punctate areas of necrotic material appear comedone-like.
- It arises from a malignant population of ductal cells.
What clinical manifestation of invasive lobular carcinoma is the LEAST likely?
- Retraction of nipple
- Bilateral lesions
- Frequent metastasizing to the CSF, ovary, uterus, and bone marrow
- Often has a diffusely invasive pattern
- Multicentric lesions
Which of the following is NOT a poor prognostic factor in the setting of medullary carcinoma?
- Polyploidy
- High nuclear grade
- Overexpression of HER2/neu
- Absence of hormone receptors
- Increased tumor size
Which of the following is a type of breast carcinoma that is MOST likely to present with fissures, ulcerations, and oozing from the nipple and areola area?
- Paget’s disease with ductal carcinoma
- Lobular carcinoma in situ
- Phyllodes tumor
- Invasive lobular carcinoma
- Medullary carcinoma
Author of lecture Breast Cancer Classification

Carlo Raj, MD
Customer reviews
3,2 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
2 |
Always enjoy lectures by Dr. Raj. Very informative and one of my favorite lecturers.
there is a higher difficulty to understand english for non-english people like me i prefer other professor.
The lectures are pretty straight forward and interesting. I enjoy the fact that other aspects are always linked in Dr Raj's lectures.
most of Dr. Raj lectures are very bad presented (( i dont like it at all ))
