Playlist
Show Playlist
Hide Playlist
Brachial Plexus Blocks – Other Limb Blocks and Intravenous Regional Anesthesia

-
10 -Other limb Block.pdf
-
Download Lecture Overview
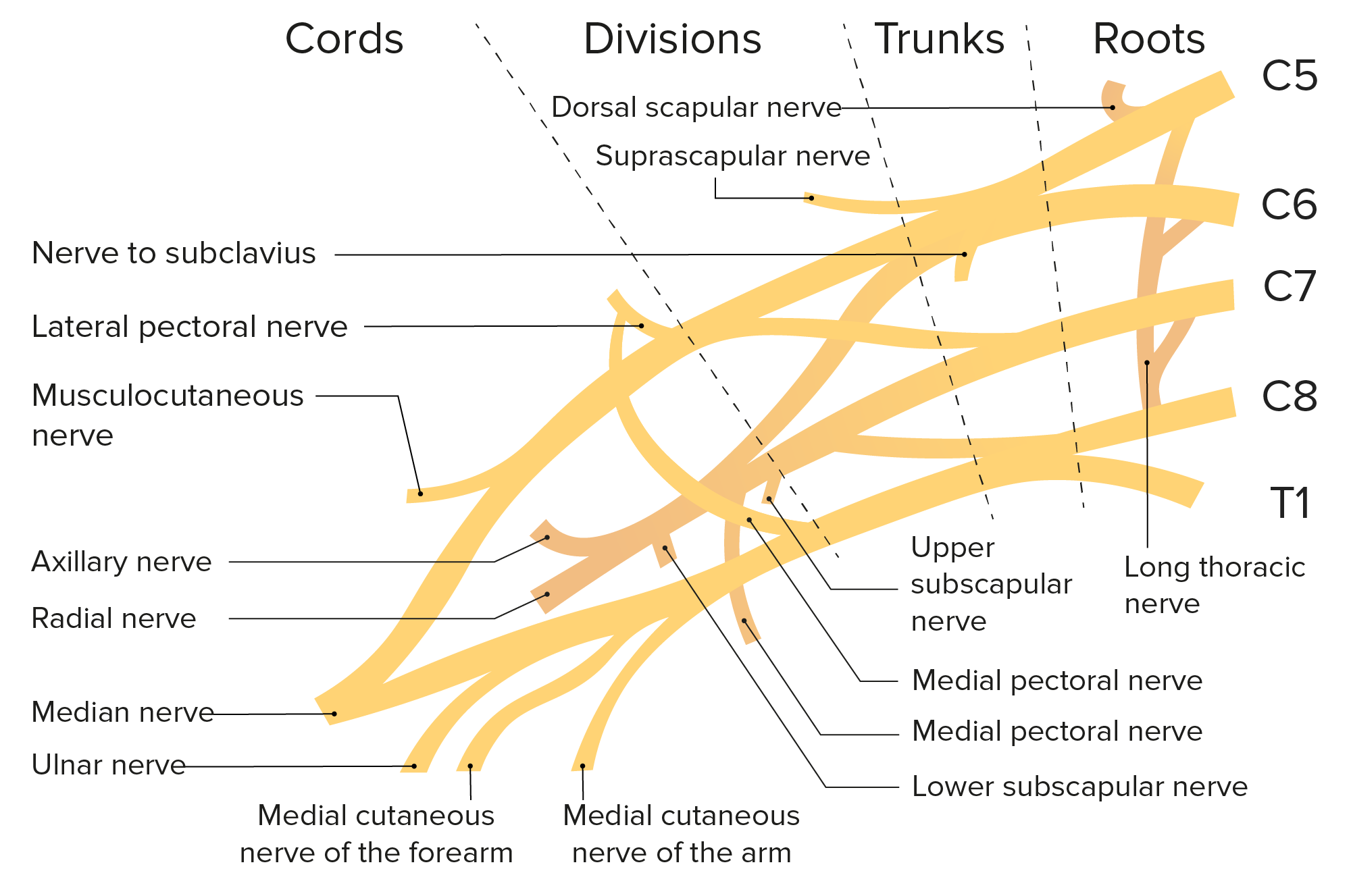
00:00 Vincent Chan in Toronto. Brachial Plexus for the upper limb, you can see in this diagram how complicated the brachial plexus is, as it comes from the neck, out through the shoulder area and down into the arm. And we're going to describe very briefly blocks in the upper limb that can be done. An interscalene approach, which is actually in the neck. 00:22 A Supraclavicular approach, which is from above the clavicle. An Infraclavicular approach, which is just below the clavicle. And an Axillary approach, which is through the, through the armpit. 00:34 And these are the areas that can be blocked. And each of these nerves, can be blocked using one of these techniques, but each of these techniques has certain areas that it blocks better than others. 00:46 So the Infraclavicular block, which is shown in this picture here, you can see the clavicle has been drawn and that the anesthesiologist is placing the needle below the clavicle. That's an lnfraclavicular block. It's a good block for elbow, forearm, and hand surgery. 01:08 The infraclavicular approach has the advantage of preserving pulmonary function by avoiding a block of the diaphragm. 01:13 A Supraclavicular block, so you go above the clavicle a little bit more towards the midline, you get excellent blocks of the elbow, arm, forearm and the hand. The Interscalene block, which is in the neck up at the level of the cricoid cartilage at C6, is a little bit riskier and we'll describe why in a couple of moments. But it's a really good block for shoulder and elbow surgery. The shoulder surgery is extremely painful post-operatively. So this is a great block either for surgery, but more commonly for analgesia after surgery. The Axillary approach through the armpit is what we used to do and it's not as reliable as the other blocks. It's not a bad block if you're lucky with it and get it for the forearm and hand, but it's not as reliable as the other blocks, so it's not widely used anymore. The interscalene block can result in a total spinal block. 02:09 So this is why it's a little riskier than the other blocks. And the total spinal block basically results in complete loss of sensation from almost the eyebrows to the bottom of the feet. 02:21 And this is a very serious complication because it blocks the entire sympathetic nervous system, as well as all the sensory and motory nerves. And the patient can't breathe, the blood pressure plummets and that's a major issue. But we can deal with it if it happens. The other problem with an Interscalene block although it doesn't usually happen, but it's possible to get a Pneumothorax, a punctured lung. It's common to get a Phrenic nerve block. The Phrenic nerve is the nerve that supplies motor function to the diaphragm and the nerve comes off of C3-C5, and goes down all the way to the diaphragm and provides the motor control of the diaphragm. So, with an Interscalene block you always get a Hemidiaphragmatic paralysis. So the diaphragm on that side is always paralyzed. This is not usually a problem, but if you've got a patient who's got respiratory problems, particularly chronic obstructive lung disease where they need a lot of muscle activity, both to inspire and expire, this can be a problem. 03:28 You never do it on both sides because you'll completely block both diaphragms in that situation. 03:34 Horner syndrome, which is a block of the sympathetic nervous system to the face, also is common. And this causes pupils to become very constricted. You get a congested nose and loss of sensation on the side of the face. It's not a serious problem, it gets better in a relatively short period of time, but it's typical of what happens with an Interscalene block. The commonest complication with a Supraclavicular block is Pneumothorax, again puncture the lung. And this can occur in up to 6% of patients. Horner syndrome occurs commonly with this block. And phrenic nerve block, an occasional arterial hemorrhage can occur. The problem with arterial hemorrhage in this situation and in the inferior clavicular block is that the artery that's bleeding is the Subclavian artery and it's very hard to put pressure on that artery because it's under the clavicle. So that can be a problem. The block should be avoided in patients with respiratory disease because of the phrenic block. The Infraclavicular block can also cause Pneumothorax and arterial hemorrhage. And both are relatively uncommon fortunately, but it can occur. They also can cause, it also could cause phrenic nerve paralysis. 04:52 The Axillary approach is more likely to cause nerve damage, because there's a great variety of nerves in that area, and it's also common to get bleeding and infection in the Axillary block. So, it's not used as much as it once was.
About the Lecture
The lecture Brachial Plexus Blocks – Other Limb Blocks and Intravenous Regional Anesthesia by Brian Warriner, MD, FRCPC is from the course Anesthesia.
Included Quiz Questions
In which of the following surgeries would infraclavicular block be used when anesthesia is required?
- Elbow, forearm, and hand surgeries
- Elbow and forearm surgeries
- Elbow and wrist surgeries
- Arm, forearm, and shoulder surgeries
- Shoulder, forearm, and hand surgeries
In which of the following surgeries would supraclavicular block be used for anesthesia?
- Elbow, arm, forearm, and hand surgery
- Elbow, arm, and forearm surgery
- Forearm and hand surgery
- Elbow and arm surgery
- Arm and forearm surgery
What is the complication of intrascalene block?
- Total spinal block
- Hydrothorax
- Vagus nerve block
- Argyll Robertson pupil
- Severe headache
Author of lecture Brachial Plexus Blocks – Other Limb Blocks and Intravenous Regional Anesthesia

Brian Warriner, MD, FRCPC
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
