Playlist
Show Playlist
Hide Playlist
Non-hormonal Regulators: Bisphosphonates, Fluoride and Calcimimetics – Bone and Calcium Medications

-
Slides Non-hormonal Regulators Bisphosphonates Fluoride Calcimimetics Bone Calcium Medications.pdf
-
Reference List Pharmacology.pdf
-
Download Lecture Overview
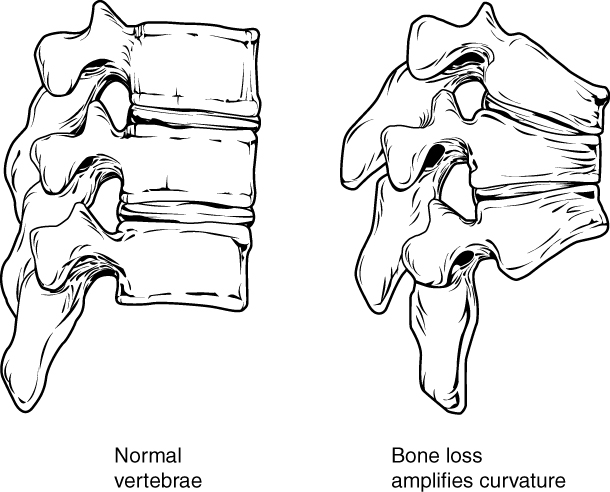
00:01 There are non-hormonal means of regulating bone mineral homeostasis. 00:06 One of the most commonly utilized in pharmacology is the bisphosphonates. 00:11 Now, bisphosphonates follow a general structure which I've shown here with variations in the R1 and R2 moieties that make up the different drugs. 00:20 The most commonly used bisphosphonates include alendronate, risdrinate, ibendronate, zoldronic acid, and pamidronate. 00:27 I won't go into the differences between all of them, I'll just talk about them as a group. 00:32 We have several indications for bisphosphonate therapy. 00:35 The most common, of course, is osteoporosis, and in particular postmenopausal osteoporosis. 00:41 That makes up the bulk of patients who receive bisphosphonates. 00:45 But it can also be used in Paget's disease of the bone. 00:48 We can also use it in bone metastases and neoplastic fractures. 00:53 We use it in the treatment of hypercalcemia. 00:55 It is used in patients who have multiple myeloma, who of course have hypercalcemia as well. 01:01 And finally, we use it in a disease called osteogenesis imperfecta, where patients have very weak and brittle bones. 01:08 Now, this is actually one of my patients. 01:10 She has blue sclera, which is one of the clinical hallmarks of osteogenesis imperfecta. 01:16 This woman is on a tidronate, and she's doing quite well. 01:19 She had possibly 30 to 40 different fractures in her lifetime prior to seeing me. 01:25 Once we started her on bisphosphonate therapy and some other therapies as well, she's actually done wonderfully well. 01:32 And in the 10 years that I've started seeing her, she's only had one further fracture. 01:36 So I think it's been a real improvement for her. 01:40 Bisphosphonates are structurally similar to a molecule called pyrophosphate, but their activity inhibits the enzymes that use this pyrophosphate. 01:51 Bisphosphonates bind very tightly to calcium, and they bind tightly in the bone itself, and they interfere with the osteoclast, which is an important cell that breaks down bone. 02:02 Bisphosphonates in general have 50% renal excretion, and they're very tightly bound to bone tissue, which gives them a very high volume of distribution. 02:13 So take another look at our original pharmacology lectures in pharmacokinetics and review volume of distribution, and you'll see why this is the case. 02:23 Now the elimination is very, very long. 02:26 It's up to decades to get rid of this product out of your body. 02:30 That makes sense because it's bound to bone. 02:33 There are a number of adverse side effects associated with bisphosphonates. 02:37 They can include stomach and esophageal erosions and ulcers. 02:41 You can get a flu-like illness from this medication, and you can get something called osteonecrosis of the jaw. 02:48 Now let's suppose your patient is going for dental surgery, and you want to start them on a bisphosphonate. 02:54 It would be wise to delay using this medication until after the dental surgery is done. 03:01 If the patient is going to have dental surgery and they've already been on a bisphosphonate, because there's such a long half-life in this drug category, it's kind of hard to justify stopping the medication. 03:13 But if you're going to start it and you have an inkling that they're going to go for dental surgery, just hold off. 03:20 Two of these drugs are associated with atrial fibrillation risk. 03:24 So this is something that we also have to consider when we're starting the medications. 03:28 In terms of long-term risk, there's something unique called bisphosphonate fractures. 03:33 So you can see here a fracture in one of my patients. 03:36 This person had a fracture of their diaphysis, and it was a particularly concerning side effect of bisphosphonate therapy. 03:46 So it seems counterintuitive that this can happen, but it is something that can occur. 03:52 Here is a list of some commonly prescribed bisphosphonates for osteoporosis. 03:57 A lendronate, known as Phosomax, is available in tablet and oral solution forms. 04:03 Next on the list is Rhizodrenate, marketed as Actinol. 04:07 This medication comes in tablets and delayed release tablets. 04:10 There are several others, including the last two listed on the slide. 04:14 When administering these medications, it's crucial to take them with water on an empty stomach and remain upright for at least 30 minutes post-dose. 04:24 Additionally, avoid eating, drinking anything other than plain water, or taking other medications for at least 30 minutes after ingestion. 04:38 I'm going to put another, I won't say drug, but let's say element in here called fluoride. 04:45 Fluoride is extensively used in dental health. 04:48 Medical doctors don't use it so much, but you see dentists using it all the time. 04:53 It does not appear to be effective in postmenopausal osteoporosis, but it is highly effective in dental health. 05:01 It may increase bone density though, we're not really sure, but we do know that there's no reduction in bone, large bone fractures with fluoride treatment. 05:10 There is no question though that fluoridation of community water sources is an effective means of reducing dental infections, including dental caries. 05:20 And we know that fluoridation of water does not cause harm despite, let's say the political craziness of today's society in believing that fluoride is somehow poisoning patients. 05:35 Fluoride does not cause significant harm in the population according to the science, and it's definitely helpful for dental health. 05:47 We have calcium mimetics. 05:49 These calcium mimetics mimic the action of calcium inside the human body, and they can be used for calcium homeostasis. 05:56 So calcium mimetics mimic the action of calcium on tissues. 06:00 They are allosteric activators of calcium, sensing receptors in the parathyroid gland. 06:07 What that gives you is a reduced output of parathyroid hormone. 06:12 So if you have high parathyroid levels, you can give a calcium mimetic to stimulate the receptor to tell the parathyroid hormone to turn off. 06:23 We use this obviously in secondary parathyroidism, especially in patients who have chronic kidney disease. 06:30 Hypercalcemia is also a disease that we treat, but only in patients who have parathyroid carcinoma. 06:39 The adverse effects, obviously a drug that's designed to reduce calcium levels can cause severe hypocalcemia, so you have to be careful to monitor the levels. 06:48 You may also get some adynamic bone disease because you're closing down the rebuilding of the bone and you can get a fracture. 06:56 You can also have nausea and vomiting from these agents because they are GI toxic for sure. 07:02 In terms of the uses of calcium mimetics, there's one drug called synacalset, which is effective to maintain levels by mimicking calcium right at the parathyroid gland. 07:15 Edicalcitide is another calcium mimetic that treats secondary hyperparathyroidism in patients with chronic kidney disease, and in fact, it's often given at the end of a dialysis session because this particular drug is fully dializable. 07:34 It may be given concomitantly with vitamin D to maintain calcium levels.
About the Lecture
The lecture Non-hormonal Regulators: Bisphosphonates, Fluoride and Calcimimetics – Bone and Calcium Medications by Pravin Shukle, MD is from the course Endocrine Pharmacology.
Included Quiz Questions
Bisphosphonate is the most appropriate treatment for which of the following conditions?
- Osteogenesis imperfecta
- Osteonecrosis of the jaw
- Osteochondroma
- Plantar fasciitis
- Frozen shoulder
What is the main mechanism of action of bisphosphonates?
- Osteoclast inhibition
- Osteoblast inhibition
- Osteoblast and osteoclast activation
- Osteoclast activation
- Osteoblast activation
What is a rare long-term (> 7 years) adverse effect of bisphosphonate therapy?
- Fractures
- Flu-like illness
- Atrial fibrillation
- Diarrhea
- Esophageal erosions
Author of lecture Non-hormonal Regulators: Bisphosphonates, Fluoride and Calcimimetics – Bone and Calcium Medications

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
