Playlist
Show Playlist
Hide Playlist
Anticoagulant Drugs – Thrombosis and Anti-Thrombotic Therapy

-
Slides Thrombotic disorders.pdf
-
Reference List Hematology.pdf
-
Download Lecture Overview
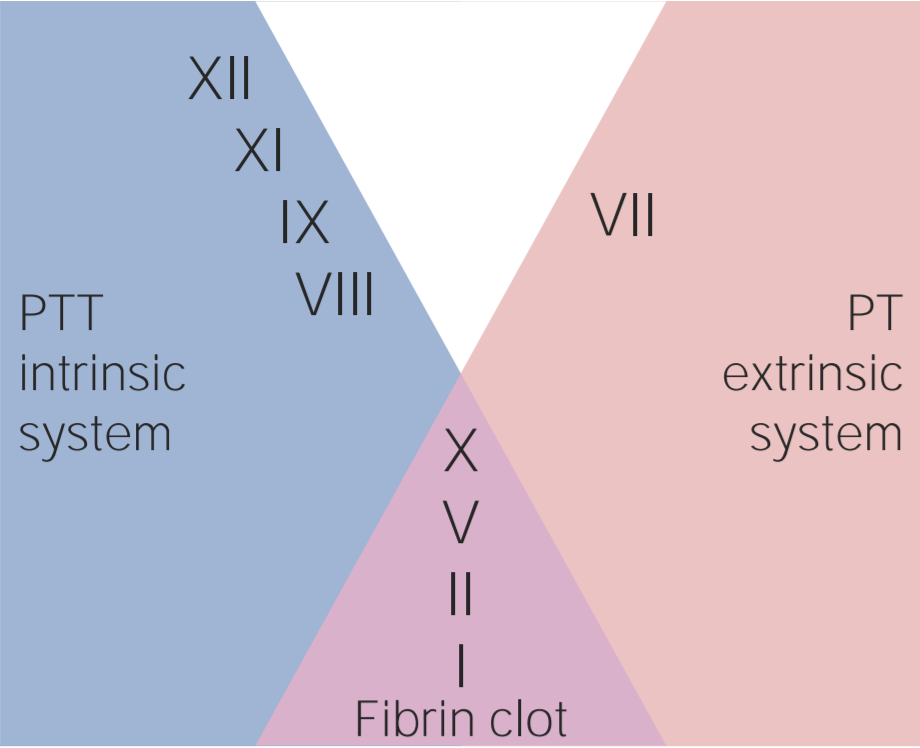
00:02 There are many drugs that have been developed for use as anticoagulants to prevent venous thrombosis. 00:10 Here are some of them, heparin, warfarin, the oral anticoagulants and antiplatelet agents. 00:18 And we'll talk about each of these in more detail. 00:22 They also want to mention physical methods to prevent thrombosis. 00:27 These are widely used and highly effective. 00:30 One is the use of support stockings for the legs. 00:34 And many patients who are admitted to hospital have these applied. 00:38 Some people use them when they go on airplanes for long plane journeys. 00:44 And at the bottom, something more invasive, but also effective. 00:49 Sometimes in patients need an inferior vena cava filter. 00:54 If they have clots in the legs, and these clots are traveling up the veins threatening the lungs, you can put a filter in the inferior vena cava to block their movement. 01:06 It can be quite effective. 01:10 Heparin. 01:11 Heparin is very widely used in modern medicine. 01:15 It's a mucopolysaccharide, but it can't be orally ingested and therefore has to be injected either intravenously, or subcutaneously. 01:25 And its activity is to increase anti-thrombin activity. 01:30 Antithrombin is not only active against thrombin itself, but a range of coagulation factors. 01:36 It's an important anticoagulant. 01:39 There are two major forms of heparin. 01:42 The most common form these days, it's called low molecular weight heparin. 01:47 You can see the molecular weight that it is 2000 to 10,000 kDa. 01:52 And it's widely used as prophylaxis to prevent or indeed as treatment for thrombosis. 02:01 Often given as a subcutaneous injection once a day, without monitoring of the blood test. 02:09 Many many patients who get admitted to hospital for whatever reason, are now given low molecular weight heparin injections to prevent the development of thrombosis. 02:20 The older, original form of heparin is the standard unfractionated heparin, and this is given as an infusion or as regular injection. 02:29 We used to use this and still do, in some situations to increase the APTT. 02:36 That's the clotting time that we use with certain effect. 02:39 But one of the beauties of this heparin is you can slow and stop and reduce it, and titrate it in need of the patient. 02:47 That can be very useful, perhaps, if a patient is going for an operation in a few hours. 02:52 Warfarin has been used widely in medicine for the past few decades. 02:57 It's a tablet which acts as an antagonist vitamin K. 03:02 And as you'll see on the top left, several coagulation factors, II, VII, IX, and X, are dependent on vitamin K for their activation. 03:13 Let's just take a time to look at that diagram on the right, and you'll see on the top left in pale color that these coagulation factors are initial inactive after they've been synthesized by the liver and they need to go, undergo, something called Gamma-glutamyl carboxylase Oxygen has to come in and this carboxylation event takes place. 03:42 Then they're activated and combine calcium, and take part in the coagulation cascade. 03:48 And you'll see that vitamin K is very important in this process of carboxylation, but it needs to be reduced again to be activated for reuse, and warfarin actually inhibits vitamin K epoxide reductase. 04:09 So, vitamin K leads to a decrease on the top right, the activated factors of II, VII, IX, and X. 04:17 Now, warfarin tends to be given for several months after patients have had an episode of thrombosis. 04:26 It will probably be easier to take a tablet every day than to have injections of heparin, for instance. 04:32 But also, patients who had heart valves, particularly older heart valves which are mechanical, they need warfarin for life. 04:42 And warfarin was a key factor in leading to the success of cardiac operations. 04:48 It's also used very often in patients who have an irregular heartbeat, atrial fibrillation, cuz that can predispose people thrombosis. 04:58 The problem with warfarin is that you need to constantly check how much you're giving by titrating it against the blood test. 05:08 That blood test is the prothrombin time, also known as the INR, the international normal ratio. 05:15 So, initially, when you start someone on warfarin, you might test this every few days, but hopefully when a patient is stable, you can test it every few weeks. 05:26 Here, we have a range of clinical indications on the left and on the right, the target INR that you might aim for with these conditions. 05:40 There you can see a deep vein thrombosis, perhaps in the legs, you might want to go for an international normal ratio of 2.5. 05:50 That means the prothrombin time is 2.5 times higher than the control within the laboratory. 05:57 And you can see by working down those indications, there's sorts of areas where warfarin can be useful in clinical practice. 06:08 However, what's quite interesting in the current time is that we're now getting a range of new tablets which can act as oral anticoagulants and these may well replace warfarin and heparin in certain situations. 06:23 These have a direct action on components of the hemostasis system. 06:29 And as we'll see in a minute, one of the advantage is, they don't need monitoring in many situations. 06:36 Look at the diagram. 06:39 We've got the coagulation pathway from the tissue factor, VIIa complex, which is the great initiator of coagulation to activation of X and the amplification through factor IX, leading to activation of X and Xa. 07:00 And of course, when X is activated, we can activate thrombin and fibrin. 07:05 And you can see down this cascade, where these these drugs have been targeted. 07:11 Many of them inactivate factor Xa or inhibit Xa. 07:17 Rivaroxaban, apixaban, edoxaban. 07:22 Whereas at the bottom, dabigatran is a IIa inhibitor. 07:28 So, acting at a slightly different point in the pathway. 07:32 Now, some of the advantages of these agents over warfarin include they're generally predictable in the dose that you can give to patients. 07:42 Blood test don't need to be done for monitoring of the patient and there's a low need to adjust the dose. 07:50 Fewer interactions with food and fewer action -- interactions with other drugs. 07:56 Although there is some concern that the reversibility of these drugs if a patient has an acute bleed. That can be difficult. 08:05 Finally, I want to mention fibrinolysis. 08:08 We can't just talk about the creation of fibrin in a platelet, the clot, without talking about how it's dissolved. 08:17 And the body, of course, has very sophisticated systems to dissolve established clots. 08:22 This is called fibrinolysis. And you'll see on the right how this is achieved. 08:29 A protein called plasminogen needs to be activated. We need to generate plasmin. 08:35 Plasmin can then break down fibrin and fibrinogen into those things called fibrin degradation products. 08:44 How is plasminogen activated? Well, by a range of molecules, and you can see them at the top, plasminogen activators. 08:53 The most important one is tissue plasminogen activator, which is released from vessels at the time of injury. 09:02 There are also other factors there. 09:05 Urokinase, which is isolated from urine, and an important one, streptokinase, which is a bacterial product being widely used in medicine over the last few years. 09:17 So, these agents are proven very effective in cases of acute thrombosis, such as acute myocardial infarction, heart attack, or perhaps the very severe pulmonary embolism, when the patient's life is at stake. 09:34 And so, you can inject tissue plasminogen activator, streptokinase, or urokinase, and they can directly lead to the dissolution of the clot. 09:45 Of course, there is a risk of bleeding associated with this agent, but used appropriately, the balance of risk is in favor of the administration. 09:55 Finally, let's look at anti-platelet drugs because these are so widely used every day at the current time. 10:03 Aspirin, this inhibits cyclo-oxygenase and that leads to reduction in the production of thromboxane, and if you take an aspirin, that will inhibit your platelets for several days. 10:16 It's an irreversible step. Clopidogrel is another widely used agent which blocks the binding of ADP to its receptor. 10:27 ADP is very important in platelet aggregation and release. 10:31 Dipyridamole, which is a phosphodiesterase inhibitor and modulates the cyclic AMP level within the platelet. 10:40 Let's use our knowledge of thrombosis and antithrombotic therapy to overview hemostasis and see how these fit into the response to vessel damage. 10:50 At the top, we see damage to the vessel wall and the three major responses to this. 10:57 Going downwards, platelet adhesion, aggregation, and release. 11:02 On the left, vasoconstriction. And on the right, activation of the coagulation cascade. 11:09 And that leads, as you'll see at the bottom, to the stable hemostatic plug. 11:14 We've seen in this lecture, how patients who are deficient in protein C or protein S, or who carry the factor V allele, factor V Leiden, are more prone to thrombosis because of their inability to inactivate activated coagulation factors. 11:34 We've seen how heparin and warfarin are also important in inactivating coagulation factors. 11:41 And we see in the center, the important role of anti-platelet agents in reducing the risk of thrombosis. 11:50 In summary, arterial and venous thrombosis are major clinical problems in current medicine. 11:56 Inherited thrombophilia and a range of environmental conditions can increase the risk of thrombosis. 12:05 Heparin, warfarin, and aspirin are well-established, they're used widely for the prophylaxis and treatment of thrombosis. 12:14 But excitingly, a range of new oral treatments is now available which may replace those agents in many situations. 12:22 I hope you've enjoyed this lecture.
About the Lecture
The lecture Anticoagulant Drugs – Thrombosis and Anti-Thrombotic Therapy by Paul Moss, PhD, OBE, FMed, FRCPath is from the course Hematologic Disorders.
Included Quiz Questions
Which of the following is a physical method of preventing venous thrombi from migrating to the lungs?
- Inferior vena cava filter
- Anti-platelet agents
- Oral anticoagulants
- Warfarin
- Heparin
To what class of molecules does heparin belong to?
- Mucopolysaccharides
- Proteins
- Monosaccharides
- Lipoproteins
- Lipids
Which vitamin is antagonized by warfarin?
- Vitamin K
- Vitamin B1
- Vitamin D
- Vitamin E
- Vitamin C
Which of the following is NOT a route of administration of heparin?
- Oral
- Subcutaneous
- Intravenous
- None of the options is correct.
Which of the following is the enzyme required for conversion of inactive coagulation factors II, VII, IX, and X into active factors?
- Gamma-glutamyl carboxylase
- Vitamin K epoxide reductase
- Vitamin K reductase
- Vitamin K hydrogenase
- Vitamin K epoxide hydrogenase
Which of the following drugs is a factor IIa inhibitor?
- Dabigatran
- Rivaroxaban
- Apixaban
- Edoxaban
- Clopidogrel
Which of the following is NOT a plasminogen activator?
- Dipyramidole
- Urokinase
- Streptokinase
- Kallikrein
- Factor XIIa
Which of the following is an ADP receptor antagonist?
- Clopidogrel
- Aspirin
- Dipyridamole
- Argatroban
- Streptokinase
Which of the following plays a role in the lysis of fibrin?
- Plasmin
- Plasminogen
- Protein C
- Protein S
- Factor V leidin
Author of lecture Anticoagulant Drugs – Thrombosis and Anti-Thrombotic Therapy

Paul Moss, PhD, OBE, FMed, FRCPath
Customer reviews
3,7 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
2 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Thank you for this succinct lecture. Key highlighted areas are great, particularly coverage on novel anticoagulants and DOACs
2 customer reviews without text
2 user review without text
