Playlist
Show Playlist
Hide Playlist
Amyloidosis – Secondary Nephrotic Syndrome

-
Slides Nephrotic Syndromes.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
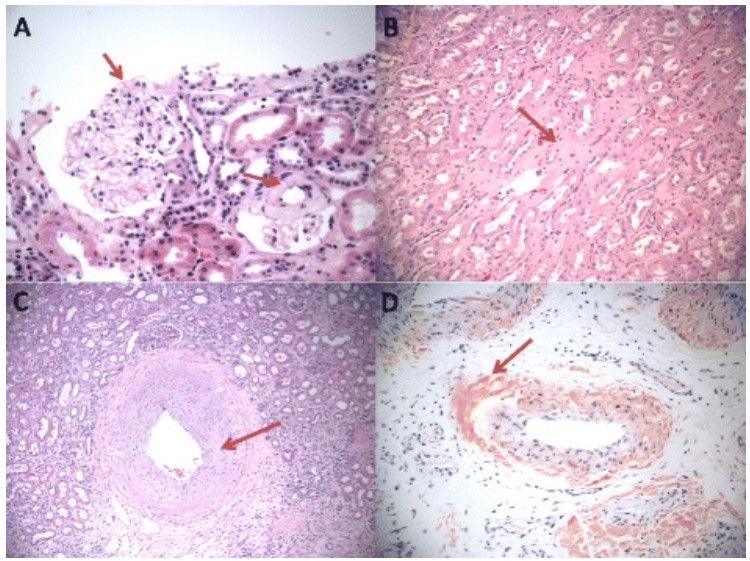
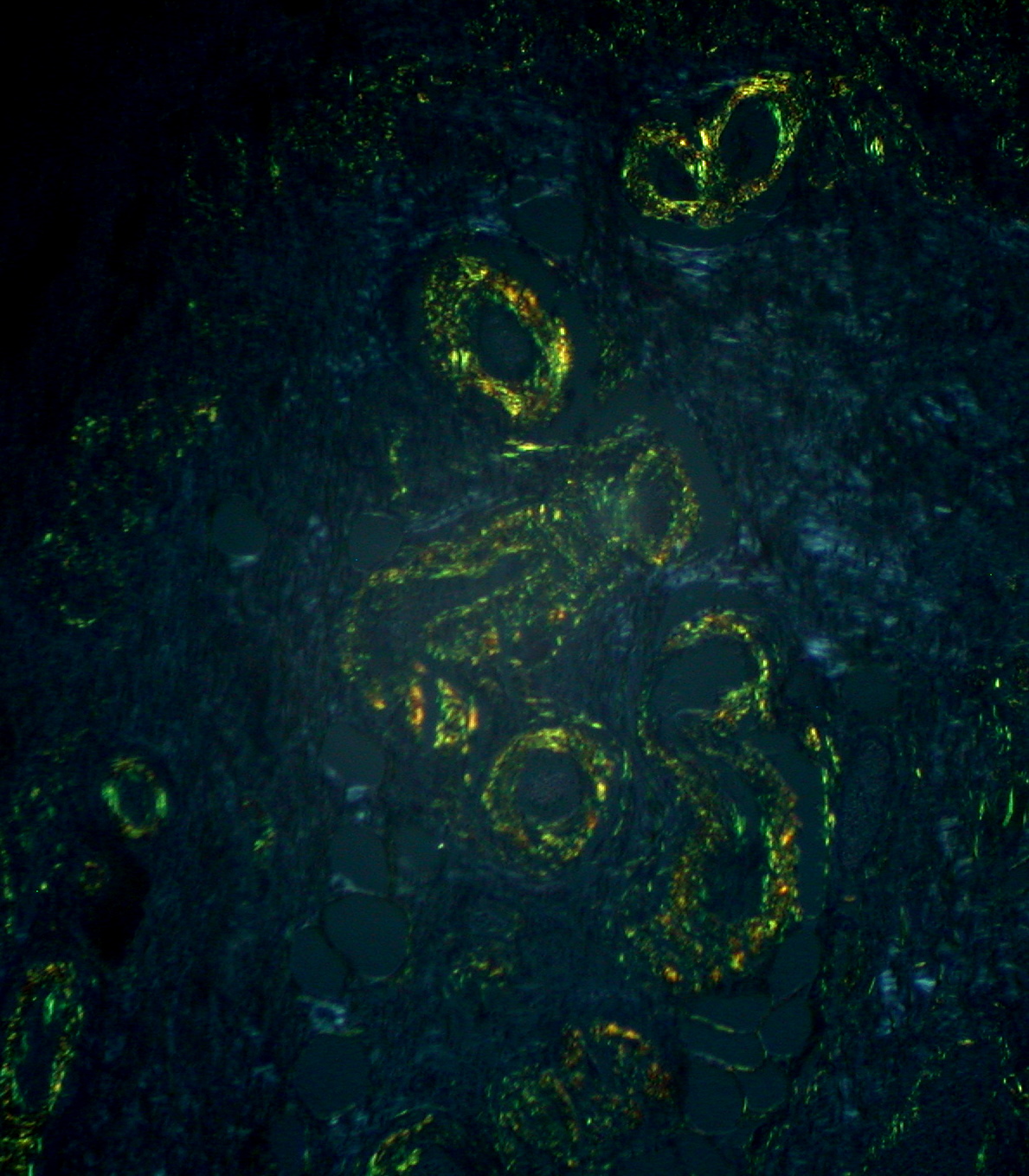
00:01 Okay, so we've concluded talking about our primary glomerular diseases or immune-mediated podocytopathies. 00:09 Let's now talk about systemic diseases where remember that podocyte is injured but it's not really playing the prominent role it's actually consequent to the systemic disease. 00:19 So these include diseases like amyloidosis, diabetic nephropathy, and systemic lupus erythematosus, which are we're going to save for a nephritic syndrome lecture. 00:31 Let's talk a little bit more about amyloidosis. 00:34 This is a group of diseases characterized by extracellular deposition of beta sheet fibrils. 00:39 That means that proteins are abnormally folded. 00:43 In the systemic form amyloid deposits in organs leading to dysfunction and eventual death. 00:49 There's over 30 proteins that are capable of amyloid formation that have been identified already. 00:56 The clinically evident renal involvement is mainly seeing with what we call AL Amyloid or AA amyloid. 01:02 However, there's been recent recognition of Lect2 in our Latino population. 01:10 So primary or AL amyloid is typically associated with plasma cell dyscrasia or plasma cell myeloma. 01:16 That's where we have abnormal proteins comprised of immunoglobulin light chains, typically it's going to be lamba. 01:23 In our secondary or AA amyloid. 01:25 These are inflammatory diseases things like rheumatoid arthritis, ankylosing spondylitis or chronic pyogenic infections typically that we may see with those who are using IV drugs. 01:38 And this is really made up of an abnormal protein serum amyloid A. 01:42 And I just want to make a comment about rheumatoid arthritis and ankylosing spondylitis. 01:46 I have to say that within the last 20 years, we've really seen a reduction in those patients presenting with AA amyloid probably because of the advent of biologic therapies and disease-modifying drugs. 01:59 It's been incredible, and we've really seen that reduction over time, which is really gratifying. 02:04 All right. So how do we diagnose amyloid? Serological tests can be very helpful with a primary for more AL amyloid. 02:11 So I want to order a serum protein electrophoresis or SPEP. 02:15 With serum immunofixation, in that patient population, I'm looking for those clonal immunoglobulin light chains that are being formed. 02:24 A renal biopsy is going to be critical. 02:26 I can't make that diagnosis without it. 02:29 A bone marrow biopsy may be warranted for anybody with AL amyloid or plasma cell myeloma. 02:36 Those amyloid fibrils of course are going to be able to bind Congo red and that leads to an apple green birefringence under polarized light. 02:43 So that's very helpful in making that diagnosis. 02:46 And they have a very characteristic appearance on electron microscopy. 02:50 Their little fibrils that are haphazardly arranged, and there are approximately 8 to 10 or 9 to 11 nanometers in diameter. 02:57 So just thinking about pathologically my light microscopy as well as my EM are going to be very important to get. 03:05 So take a look at what this looks like pathologically. 03:07 Again, let's look at our normal glomerulus, do we just remember what it looks like. 03:11 I want you to appreciate how those capillary loops are open and beautiful very delicate looking, and then we have amyloid. 03:19 So this again is a H&E staining so we can see the cells that are prominent there. 03:25 But if you look at those capillary Loops instead of being beautiful and delicate they're really filled in those mesangial areas, but this amorphous in a material, that's the amyloid. 03:35 Now if I use my Congo red stain that's going to bind to the amyloid so you can see that reddish hue that's binding the masamgial areas where amyloid has deposited. 03:45 Now if I take that and I put it under polarized light you can see that beautiful apple green birefringence. 03:51 That's the amyloid so it clenches our diagnosis for AL amyloid. 03:56 So how do we treat our patients who have amyloidosis? Again, all of those patients really should receive nonspecific therapy for the nephrotic syndrome, that's going to include our ACE inhibitors, our ARB's or Loop diuretics are low sodium diet bloodpressure control as well as hyperlipidemia treatment. 04:12 But in the primary form of amyloid, there are some things that we can do to treat our patients in the AL form. 04:17 We want to give our patients chemotherapy. 04:19 This is typically proteasome inhibitor based regimens, as well as glucocorticoids to shut down the production of those immunoglobulin light chains. 04:27 And in some cases we can do hematopoietic stem cell transplantation. 04:33 In AA amyloid, remember that's our secondary form of amyloid. 04:36 We really want to target treatment at that underlying disease process in order to reduce inflammation. 04:42 Again, as I was talking about with rheumatoid arthritis and some of our other diseases. 04:46 We have such good biological therapies that are out there and disease modified treatments that we don't see a lot of AA amyloid with that anymore fortunately.
About the Lecture
The lecture Amyloidosis – Secondary Nephrotic Syndrome by Amy Sussman, MD is from the course Nephrotic Syndrome.
Included Quiz Questions
Which of the following stains is used to identify amyloid deposits on renal biopsy?
- Congo red stain
- Periodic acid–Schiff stain
- Jones silver stain
- Hematoxylin and eosin stain
- Prussian blue stain
What is the origin of amyloid deposits in patients with rheumatoid arthritis?
- Serum amyloid A protein
- Transthyretin
- Immunoglobulin light chains
- Amyloid beta (Aβ) plaques
Which of the following is true of amyloidosis?
- Primary amyloidosis is usually treated with a proteasomal-inhibitor-based regimen and glucocorticoids.
- Secondary amyloidosis can be treated with hematopoietic stem cell transplant.
- Primary amyloidosis is usually caused by inflammatory diseases.
- The abnormal protein causing secondary amyloidosis is typically immunoglobulin light chains.
- The abnormal protein causing primary amyloidosis is typically serum amyloid A protein.
Author of lecture Amyloidosis – Secondary Nephrotic Syndrome

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
it is perfict ,simple and complete. i enjoyed it and found it helpfull.
