Playlist
Show Playlist
Hide Playlist
Amebicides – Antiprotozoal Agents

-
Slides Amebicides Antiprotozoal Agents.pdf
-
Reference List Pharmacology.pdf
-
Download Lecture Overview
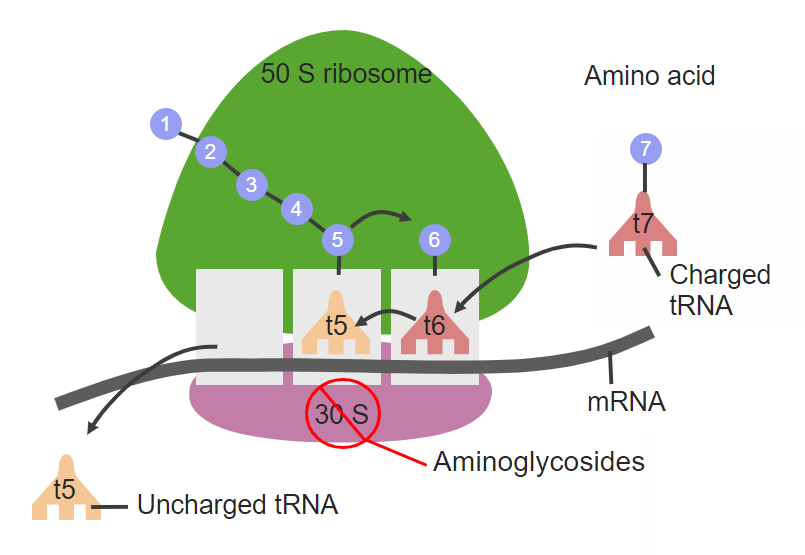
00:01 Let's move on to the amebicides. 00:02 Now amebicides are going to be divided into two different groups. 00:10 Those amebicides that act systemically in the tissues and those are for people with systemic infections. 00:16 And those amebicides that acts exclusively in the bowel. 00:19 And those are people who have more GI limited disease. 00:24 Now you can say that agents are very similar to the anti-malarial agents. 00:29 Chloroquine, metronidazole, tinidazole. 00:32 These are all agents that you've seen before. 00:34 Luminal amebicides act on organisms in the bowel lumen. 00:37 So these are the agents here that you can see that we use for luminal agents. 00:43 And we'll go through each of them in detail. 00:48 Let's start off with the emetines. 00:51 So the emetines are a group of drugs that block ribosomal movement along the messengerRNA. 00:57 So this is kind of an interesting visual idea. 01:00 Imagine that that messengerRNA is a long railroad track. 01:04 The ribosome is a kind of like a car on a train that just travels along the track. 01:09 And as it travels along the track it reads different codes in the messengerRNA and produces a protein. 01:15 The movement of that ribosome along the railroad track is blocked by this class of drugs. 01:21 And by that method inhibits proteins synthesis specially for organisms like amoeba. 01:27 In terms of toxicity, there's quite severe toxicity with these agents and it's actually extremely common. 01:35 GI distress is going to be the number one type. 01:38 You can also sometimes get muscle weakness. 01:40 And in terms of cardiac muscle, you can get arrhythmia, and congestive heart failure. 01:44 So be very aware of the side effects of these medications. 01:48 Because of these potentially severe side effects, emetine is now rarely used and is generally reserved for cases where other treatments have failed or are contraindicated. 02:00 The other agents that we use to kill, to act as amebicides are metronidazole and tinidazole. 02:07 So we have seen before in our other lectures on anti-bacterials. 02:12 The mechanism of action we belief is through bio-activation by anaerobes to form cytotoxic products. 02:19 Now there's a nitro group that's reduced by ferredoxin that can also be quite toxic too. 02:25 The drug of choice, this is the drug of choice in severe intestinal wall disease and hepatic abscesses, metronidazole in particular. 02:33 It works very well in extra intestinal diseases as well. 02:37 So I'm not suggesting that metronidazole can't be used in systemic disease. 02:41 I'm just suggesting that in terms of luminal disease and hepatic abscesses it's a very good drug. 02:48 Metronidazole is the drug of choice in trichomoniasis and several other types of amebic infections and anaerobic infections. 02:59 Tinidazole is effective against metronidazole-resistant organisms. 03:04 So it is our backup plan when metronidazole doesn't work. 03:12 Other agents that we used in the treatment for amebicide activity is dyloxanide, which is no longer available in the United States. 03:22 Now it is a luminal amebicide. 03:25 It is converted within the gut itself to the freebase form. 03:29 The freebase form is an amebicide through an unknown mechanism. 03:33 It is used in asymptomatic amebiasis. 03:36 So it's very, very effective. 03:39 It's used in mild intestinal disease in combination with other drugs. 03:44 Toxic effects are really related and limited to the bowel. 03:47 And we're talking about abdominal bloating with a lot of gas production or diarrhea. 03:54 Iodoquinol, also known as diiodohydroxyquin, is another agent that is considered luminal amebicide. It is no longer available in the US. 04:03 It is used in mild to moderate to severe infections. 04:07 So it's a whole range of infections. 04:09 Toxic effects once again are fairly limited to the bowel. 04:12 And they tend to be common but not a severe. 04:15 And people will complain of some mild abdominal bloating or they will complain about diarrhea. 04:20 Overdose symptoms. 04:22 In overdose we have to be aware of significant problems including thyroid enlargement. 04:28 Quite severe skin reactions. 04:30 And in some cases neurotoxicity. 04:33 And in terms of the neurotoxicity, one of the most feared ones is visual dysfunction which can also get a peripheral neuropathy as well. 04:45 Paromomycin is the preferred luminal amebicide and it is also an aminoglycocide antibiotic. 04:51 So we did cover it very briefly in our anti-bacterial lectures too. 04:55 In terms of toxicity, headaches, dizzines, rashes and anthralgia are very common with this class of agent and with all aminoglycocide agents. 05:05 The toxicity risk is going to be proportional to renal function. 05:10 So if a person has stage 3 renal disease, the toxicity risk is actually quite high. 05:18 So the next drug that I want to mention is nitazoxanide which is quite a good drug. 05:23 It has activity against a whole range of protozoan agents. 05:27 It works quite well against Entameoba histolytica. 05:31 It works well against the Helminths class of organisms. 05:35 It works quite well against Giardia Lambia. 05:38 And if you recall that's the one we prozactly call it the "Rocky Mountain Runs." That's where you get quite explosive diarrhea from drinking effected river water or lake water. 05:51 A bit of a note on that. 05:54 We commonly think of that being something common to the rocky mountains because of it's name. 05:59 But in actual fact it's not just limited to places like Alberta in Canada or Colorado in the United States. 06:06 It's also present in the northeast. 06:08 So it's present in Ontario in Canada. 06:11 It's present also in places like rural Pennsylvania or New York in the northen United States. 06:18 So don't just think of it as a western disease. 06:21 It's also an east coast disease as well. 06:23 We also use it against cryptosporidium. 06:26 We can also use it in other agents of protozoa too. 06:30 Now we also can use this agent in those organisms that are resistant to metronidazole which is becoming more and more common as time goes on. 06:40 So I suspect that this drug is going to become more important with time. 06:44 Now here's the overview of the treatment. 06:47 And I'll just go over it again. 06:48 And we also have the final slide as a downloadable image that you can look at yourself on your own time. 06:55 So for asymptomatic intestinal infection, the first-line drug of choice is paromomycin. 06:59 It's a very, very active agent and it works quite well. 07:03 In terms of mild to moderate intestinal infections, we move to metronidazole. 07:09 And we also add in luminal agent like the one that was listed above. 07:14 With respect to the severe intestinal infections, with or without реritοոitis or toxic megacolon, we have of course are going to use metronidazole plus a luminal agent and antibiotics against gram-negative organisms. 07:27 Now if the agent is resistant to metronidazole, we will substitute tinidazole or nitazoxanide plus a luminal agent & antibiotics. 07:36 We will always add a luminal agent with the metronidazole in symptomatic infections. 07:41 Alternatives can be tetracyclines or one of the emetines as well plus a luminal agent. 07:47 In terms of patients who have hepatic abscesses and other types of extra intestinal disease, we are going to use metronidazole plus a luminal agent & antibiotics. 07:58 Or in resistant cases we'll use tinidazole or nitazoxanide plus a luminal agent & antibiotics. 08:03 So you notice that moderate, sorry, severe intestinal disease and hepatic abscesses are treated essentially the same. 08:11 So there's the entire graphic. 08:13 We'll have that as a downloadable for you so that you can look at it on your own.
About the Lecture
The lecture Amebicides – Antiprotozoal Agents by Pravin Shukle, MD is from the course Antimicrobial Pharmacology. It contains the following chapters:
- Amebicides
- Amebicides: Overview of Treatment
Included Quiz Questions
A young woman comes to you complaining of itching in the genital area, a bad-smelling thin discharge, and dyspareunia. Which drug will be your first choice of treatment?
- Metronidazole
- Diloxanide
- Chloroquine
- Iodoquinol
- Paromomycin
Which drug is an amebicide in its freebase form?
- Diloxanide
- Chloroquine
- Metronidazole
- Iodoquinol
- Paromomycin
A patient comes to you with thyroid enlargement. He mentions recent treatment for an infection by a parasite, but can't recall the name of the medication. Which drug would be the most likely cause of the thyroid enlargement?
- Iodoquinol
- Chloroquine
- Metronidazole
- Diloxanide
- Paromomycin
Which amebicide is also an aminoglycoside?
- Paromomycin
- Diloxanide
- Chloroquine
- Iodoquinol
- Tinidazole
Which drug has activity in the bowel wall?
- Diloxanide
- Ceftriaxone
- Emetines
- Metronidazole
- Tinidazole
Author of lecture Amebicides – Antiprotozoal Agents

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
