Playlist
Show Playlist
Hide Playlist
Adenocarcinoma



-
Slides PulmonaryNeoplasia RespiratoryPathology.pdf
-
Download Lecture Overview
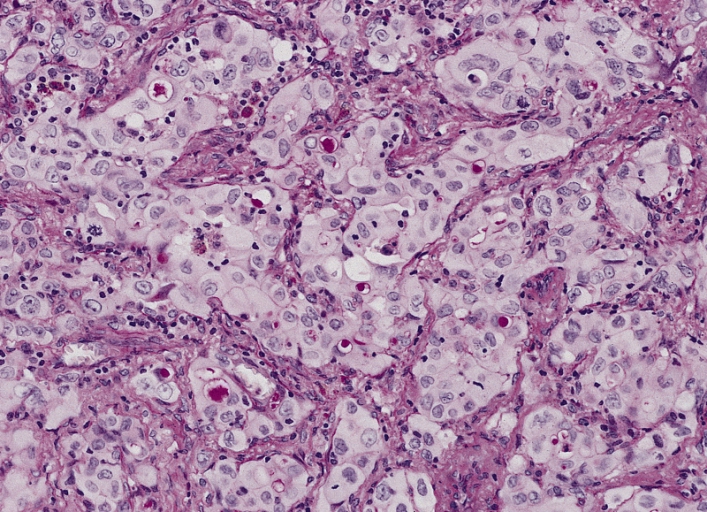
00:00 Our non-small cell lung cancer include adenocarcinoma. Let’s take a look. 00:06 Adenocarcinoma, know everything about this lung cancer. It is the most common type of lung cancer. Period. Okay. The last time we even discussed bronchogenic lung cancer, do you remember a particular pneumoconiosis that was associated with the development of bronchogenic carcinoma decades down the road? Good, maybe the patient was a roofer, a plumber, right? Maybe the patient was working in a naval shipyard. That was asbestosis. Good. And that asbestos is going to then affect what part of the lung? The basal or the upper lobe? It was really the only one of the four pneumoconiosis that was affecting the basal. So, that was our discussion back then. We’ll take a look at adenocarcinoma. 00:55 You tell me, first, a primary lung cancer, how many nodules? Good, one. This nodule, if it was small cell, was located where? By the mediastinum. How do you describe this clinically? Central. Chest X-ray for adenocarcinoma, you pay attention to peripherally located one nodule. By periphery I do not mean the pleura. Adenocarcinoma is not a cancer of the pleura. You give me a diagnosis where cancer of the pleura has taken place. It’s mesothelioma, okay? Not here. So, by peripheral let's just say away from the mediastinum, peripherally located. How many nodules? One. Why not two or three? That’s metastasis. 01:47 What’s the number 1 place for metastasis? Can’t say number 1, but give me couple of common metastasis of a primary cancer to the lung. Good, liver. Give me another one. The lung is right around, the breast. Okay, keep those in mind. 02:06 Characteristics of adenoma. We’ll walk through each point here. Most common primary lung cancer, point 1. Point 2, the activation mutations. Well in neoplasia we’ve talked about plenty of these. The one that’s most famous of them all, RAS. 02:26 Remember RAS? Associated with what? GTPase. Remember that? Bring it in here. Here RAS becomes important and you find that in many cancers. With EGFR (epidermal growth factor receptor). Last time we’ve talked about that was with breast cancer, right? Epidermal growth factor receptor. And then you have an important one. ALK. This is anaplastic lymphoma kinase. This is going to be little bit more specific for adenocarcinoma. 02:54 Luckily and conveniently, both begin with the letter A. 02:55 Next, when you have bronchogenic carcinoma, we take a look at the digits. And looks like the nail is expanded. This is called hypertrophic osteoarthropathy. We’re not exactly sure what causes this, but the bone underneath your nail, osteo, undergoes hypertrophic changes. 03:19 Literally it pushes the nail upwards. Looks like clubbing, but you don’t call it clubbing, because clubbing would be what? Clubbing would be part of chronic hypoxia, do you remember that? So here we have hypertrophic osteoarthropathy as more or less your paraneoplastic issue that you’d find with bronchogenic in a whole, but adenoma. 03:40 Now, the subtypes are important for us. We have in-situ. What’s in-situ mean to you? It means that membrane is intact. Just because the membrane is intact, does it mean that you’re not malignant? My question once again, just because the membrane is intact, in-situ, does it mean that you’re not malignant? No. You could be in-situ and still be malignant. 04:00 Welcome to the in-situs of the breast. Lobular carcinoma in-situ, right? The breast, the ductal carcinoma in-situ. Luckily the membrane has not been ruptured. 04:13 So, the adenocarcinoma in-situ is known as the bronchoalveolar subtype. It will show hazy infiltrates similar to consolidation. Be careful. Consolidation, well, you usually think about pneumonia, but there you would have fever and such. In chest X-ray maintains better prognosis. Characteristics of adenocarcinoma: be familiar with the in-situ subtype known as bronchoalveolar. 04:39 Let's take a look at histology here. Now, before I move on, you tell me what adenoma means. For example, stomach cancer – gastric adenocarcinoma. Per-rectal cancer – adenocarcinoma. 04:52 Prostate cancer – adenocarcinoma. Breast cancer – adenocarcinoma. Adenoma means what? Those are all glandular structures, aren’t they? So, glandular, tall, columnar. 05:01 Adenoma. So that’s non-specific, that just means glandular, you knew that already. 05:06 Now, pattern on histology, are they going to now stain? Once again, you have something that’s a glandular, it will be mucin positive. Okay? Mucin positive. Do you have any of that paraneoplastic craziness that we saw with small cell? We saw what? ADH, ACTH and stuff. 05:22 No, not here. So, you wouldn’t expect to find the Kulchitsky cells and the chromogranin A and neuron-specific enolase. The bronchoalveolar subtype grows along the alveolar septa. What’s bronchoalveolar? See what’s bold in here, go back to characteristics. It means in-situ. 05:40 So, subtype of this grows along the alveolar septa with apparent thickening of the alveolar wall. 05:47 Rupture? No, this is not invasive, it's in-situ. Spend time, make sure you at least know this much of adenocarcinoma before you then move on to any other lung cancer.
About the Lecture
The lecture Adenocarcinoma by Carlo Raj, MD is from the course Lung Cancer .
Included Quiz Questions
Which of the following findings on histology is associated with adenocarcinoma?
- Mucin +
- Multinucleated giant cells
- Calretinin +
- Chromogranin A
- Enolase +
What differentiates the bronchoalveolar subtype of adenocarcinoma from other types of pulmonary adenocarcinomas?
- The membrane surrounding the malignancy is intact.
- It is a benign tumor.
- It commonly affects the upper lobes.
- It is associated with clubbing of the digits.
- It causes bronchospasms.
Which of the following is associated with adenocarcinoma of the lung?
- Hypertrophic osteoarthropathy
- Osteoarthritis
- Flushing of the upper extremities
- Digital clubbing
- Hypertrophic cardiomyopathy
Author of lecture Adenocarcinoma

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
