Playlist
Show Playlist
Hide Playlist
Acute Inflammation: Signs & Symptoms – Inflammation and Wound Repair


-
Slides Inflamation Cellular Pathology.pdf
-
Download Lecture Overview
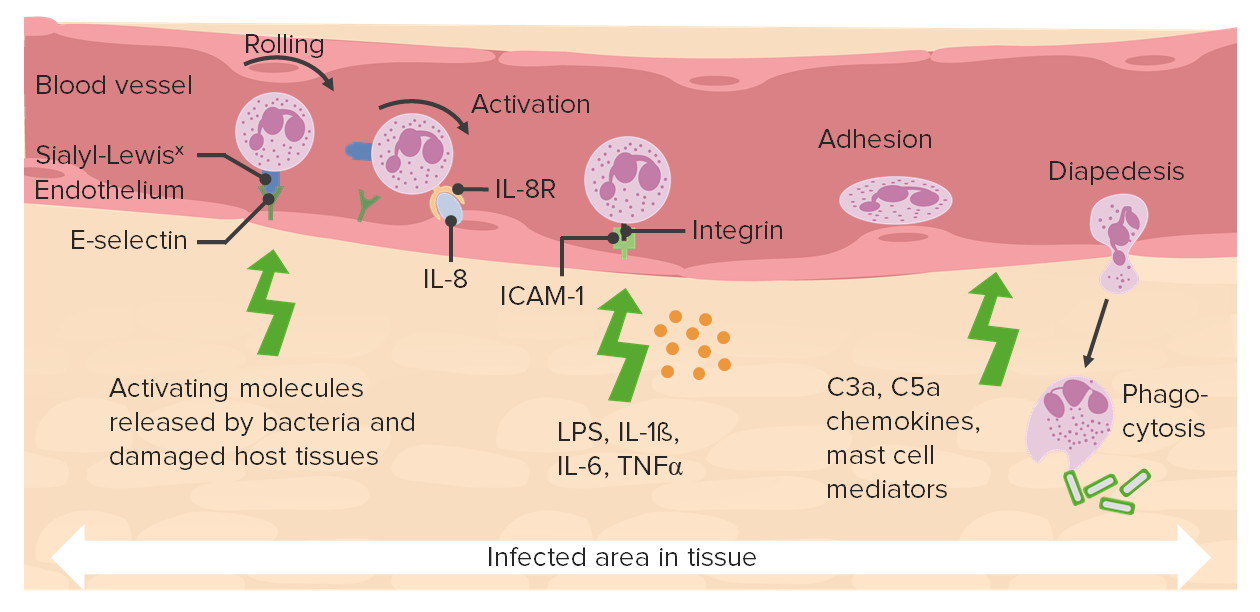
00:01 In this section of basic pathology we will take a look at inflammation and wound repair. Organization will be acute inflammatory mediators quickly reviewing that what you have seen in Immunology. Going into chronic inflammation, and a few words about wound repair. To begin with, take a look at the various cells that are involved in inflammation. 00:22 When we talk about WBC's, you should be able to identify many of this cells. Remember in acute inflammation, it's a fact that neutrophil are coming in. And neutrophils as you see in the picture are properly segmented. Not hypersegmented but definitely segmented. Approximately 4 to 6 lobes is what you are expecting to see. At some point in time, if chronic inflammation is what's occuring, then it is the monocyte that is being recruited. And you notice here that the nucleus of a monocyte should be approximately the size of an RBC and you notice that the monocyte and it's nucleus should be quite circular. 01:01 Versus for example; When you deal with infection such as viral. That will be CMV or EBV. There is every possibility that now, this monocyte then becomes what's known as an atypical monocyte. Monocyte will be in circulation. If a monocyte then ends up in your tissue you then call this a macrophage. In acute inflammation, the cardinal signs that you would expect to see would be rubor, redness; calor, heat; tumor, swelling; pause here for one second. The reason I say that is I will quickly walk you through acute inflammation and the different changes. And you have seen this before, in immuno. For example, let's say that there is an antigen, a bacteria that is now been introduced into the interstitium. What has to happen is that the neutrophil, which is the acute inflammatory cell has to move from your circulating pool over to the marginating pool. 02:08 We'll talk about quickly once again, review some of those mediators including your selectins, pherolins, integrins for proper adhesion. 02:19 And then finally getting through your endothelial cell. A process known as diapedesis. Now the diapedesis or transmigration would then get the neutrophil out in interstitium but in order for your neutrophil to get out into the interstitium, what does the blood vessel has to do? Not vasoconstrict but vasodilate. When you vasodilate, the mediator here please. 02:44 Do you remember? That's responsible for the eventual or should I say very quick vasodilation. Would be histamine. If you vasodilate are'nt you creating a inflammatory state? Sure. The swelling, the tumor. If you increase in amount of blood flow to that area, then you would expect to be increased redness. So, rubor. With increase blood flow to this area, you would also expect there to be emission of heat. Calor, think of burning calories. At this point, 3 of the 5 cardinal signs of acute inflammation; rubor, calor, tumor, is then being created by histamine on purpose. And the reason for this is because of neutrophil has to then get through the gap junction of the endothelial cell into the interstitium. 03:36 And there you will have, and we will talk about a few chemotactic factors and those opsonins. Dolor, pain. 03:45 Histamine will be the major mediator and bradykinin responsible for pain. The picture, if it's a bacterial infection, erysipelas, meaning to say that here due to that acute inflammatory response there is quite a bit of reddening that you can expect because of acute inflammation. The key cells of acute inflammation will be neutrophils. And here the dark cells that you see in this particular structure would then indicate recruitment of your neutrophils in great number. If you were to then blow up a neutrophil then you would expect to see what kind of cell? A segmented neutrophil. Remember in certain issues such as B-12 deficiency or folate deficiency in which you may then result in hypersegmented type of neutrophil which is a primitive cell. 04:38 In the very beginning of this I actually showed you a band cell. What does a band cell mean to you? It's a very primitive neutrophil. 04:46 And there should be a certain number of Band cell in circulation but if there is acute inflammation, you can imagine now that the band cell number would be increased. Do not forget that if you are dealing with neutrophils, or in general, if you are dealing with a tri-lineage of cells of your hematopoietic or your stem cells that you should be beginning from the bone marrow always. Remember neutrophil will be the most abundant type of a granulocyte or a WBC followed by eosinophils and basophils.
About the Lecture
The lecture Acute Inflammation: Signs & Symptoms – Inflammation and Wound Repair by Carlo Raj, MD is from the course Cellular Pathology: Basic Principles with Carlo Raj.
Included Quiz Questions
What cells are markedly increased in acute inflammation?
- Neutrophils
- Basophils
- Eosinophils
- Monocytes
- Lymphocytes
Why are vasodilation and swelling beneficial in acute inflammation?
- Swelling allows for the entry of neutrophils into the interstitium in order to access the infection/injury.
- Swelling allows for the pooling of immune system cells in the area of infection/injury.
- Swelling allows for monocytes to leave the circulation and transform into macrophages.
- Swelling promotes fluid movement and the clearing of pathogenic material.
- Swelling promotes the release of histamine into local tissues.
Which of the following is NOT a cardinal sign of acute inflammation?
- Fibrosis
- Redness
- Heat
- Swelling
- Pain
Author of lecture Acute Inflammation: Signs & Symptoms – Inflammation and Wound Repair

Carlo Raj, MD
Customer reviews
1,8 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
3 |
With this topic is easy to get lost ini all the details and I think he made a good overview to not forget de bi image when we get in the details
if i wanted monotoned reading i would have read textbooks instead of watching this video.
Poor presentation. It's just like he is reading out from study material. Lacks concepts.
With all the rrespect the spoken language is blurred, I can’t understand properly, plus your eyes are focus on something maybe an aid material, it would be better if instead they were focused on the camera and try to explain rather than read. Thank you for caring.
