Playlist
Show Playlist
Hide Playlist
Acute Headache: Hypertensive Urgency and Cluster Headache (Horton's Syndrome)



-
Slides 08 Headache Neuropathology I.pdf
-
Download Lecture Overview
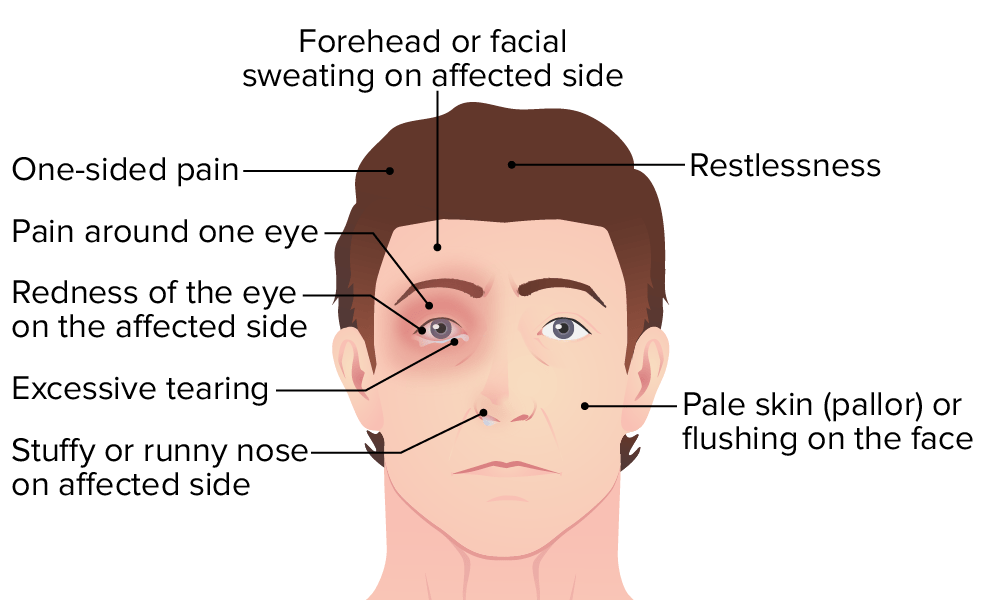
00:01 Let’s talk about hypertensive urgency as being a presentation of acute headache. 00:07 Dull, bilateral ache head pain, no focal deficit, possible diminished level of consciousness if associated with reversible posterior type of leukoencephalopathy. 00:25 Usually seen when systolic blood pressure is above 180 or the diastolic blood pressure is above 120. 00:32 Treatment here is you need to make sure that you take care of the hypertension. 00:36 Urgency versus your crisis, or emergency, and your crisis is the one in which you don’t mess around. 00:43 At that point, you need to make sure that you give IV, do everything in power in which you give IV nitroprusside to take care of the blood pressure ASAP. 00:51 Remember, we talked about hypertension urgency versus crisis. 00:56 Here, let’s talk about a cluster headache. 00:59 The duration becomes important. 01:01 Abrupt in onset, peaking approximately five to ten minutes later. 01:06 That is important. 01:08 Pay attention to that. 01:10 Persists for 45 minutes to 2 hours. 01:13 And clusters, meaning to say over days to weeks. 01:17 So it comes in these clusters, over days to weeks. 01:22 Peak of five to ten, persists for 45 minutes to 2 hours, and comes in clusters. 01:29 Consistently unilateral and orbital in location. 01:34 “Doc, it feels like I have pain in my eye. 01:38 It feels like someone is stabbing me in the eye.” Orbital location. 01:42 Pain described as deep, intense, boring, meaning to say like a needle being put. 01:48 So, they don’t call this being throbbing. 01:50 Throbbing will refer to as being our giant cell arteritis. 01:54 “Doc, I feel like these pulsations of throbbing headaches.” Boring is more like a needle, being stabbed. 02:02 These patients are moving around the room, banging their head on the wall, screaming for medication because could you imagine putting a needle into your eye? Isn’t a good feeling. 02:13 Nausea and vomiting are atypical, associated with lacrimal or nasal secretions. 02:20 Who does it occur in? Young adult men. 02:23 Usually, onset will be 30s. 02:26 Male to female ratio, males much more so than females with cluster headaches. 02:31 Now, suicide, an occasional complication. 02:35 This darn headache is so bad that that patient is not able to handle and manage this by himself or herself, most likely himself, that he wishes to then kill himself due to the intense nature and predictable recurrent rate of the pain. 02:50 That becomes important. 02:51 Even though we just call this a headache, we understand the implications can quite literally be grave. 02:58 Let’s take a look at management of cluster headache. 03:00 Abortive therapy is often ineffective due to the rapid onset. 03:04 Remember, short duration of attacks. 03:06 So the peak is five to ten minutes. 03:08 However, you say short duration. 03:10 Keep that in mind, it’s all relative. 03:12 Forty-five minutes is actually not a lot of time over a grand scheme of things. 03:18 However, for the patient, it feels like eternity. 03:21 “Doc, my headache feels like it’s forever.” Yes, when you’re in that type of pain, even 30 seconds is too long. 03:29 The first-line therapy consists of oxygen, specifically 100%, administered via a nonrebreathing facial mask at a flow rate of at least 12 liters per minute. 03:39 The second-line therapy includes triptans, such as subcutaneous sumatriptan. 03:45 It is important to note the contraindications for sumatriptan, which are ischemic cardiovascular disease, history of stroke, or uncontrolled arterial hypertension. 03:54 Third-line therapies are more varied and include intranasal lidocaine, oral ergotamine, and intravenous dihydroergotamine. 04:02 Preventive treatment for cluster headaches includes the following options: Verapamil is commonly used. Glucocorticoids are prescribed with a tapering dosage. 04:11 Among alternative options are: Galcanezumab, also known as Emgality. 04:18 This s a Calcitonin Gene-Related Peptide antagonist. 04:22 Lithium and topiramate are other medications which can be used. 04:26 A greater occipital nerve block is an interventional method. 04:30 In summary of cluster headache: Risk factors: male, much more so, young male, 30s. 04:37 Signs and symptoms: unilateral boring, boring, boring. 04:41 By boring, you know what I’m referring to now. 04:42 I’m not saying, “Well, I’m sitting on my couch watching TV because I’m bored.” No, no, no, this is boring like you’re stabbing someone. 04:53 Differential diagnosis: glaucoma, dissection, cerebral vein thrombosis. 04:58 Diagnostic workup: H&P, image can rule out other diagnoses if it’s causing this type of headache. 05:07 Otherwise, H&P. 05:09 For acute treatments, we discussed oxygen, triptans, intranasal lidocaine, and ergotamines. 05:17 For prevention, you can use verapamil, glucocorticoids, galcanezumab, lithium, topiramate, or a greater occipital nerve block.
About the Lecture
The lecture Acute Headache: Hypertensive Urgency and Cluster Headache (Horton's Syndrome) by Carlo Raj, MD is from the course Headache – Pathophysiology. It contains the following chapters:
- Acute Headache: Hypertensive Urgency
- Acute Headache: Cluster Headache
Included Quiz Questions
Which of the following statements is TRUE regarding the nature and location of pain in cluster headaches?
- Stabbing and unilateral pain associated with tearing
- Stabbing pain located in the occipital area
- Throbbing and unilateral headache
- Dull band-like pain around the head
- Unilateral headache associated with nausea and vomiting
What is TRUE regarding a headache due to severe hypertension?
- The focus of treatment is to control the patient's hypertension.
- The focus of treatment is anticoagulation.
- The focus of treatment is to control pain and not be concerned with blood pressure.
- The patient usually presents with neurologic findings.
- The patient usually presents with a unilateral throbbing headache.
Author of lecture Acute Headache: Hypertensive Urgency and Cluster Headache (Horton's Syndrome)

Carlo Raj, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Well explained. The failure was to be so explicit without a lot of explanation.
