Playlist
Show Playlist
Hide Playlist
Acute Disseminated Encephalomyelitis, Transverse Myelitis and Central Pontine Myelinolysis

-
Slides 01 Multiple Sclerosis Neuropathology II.pdf
-
Download Lecture Overview
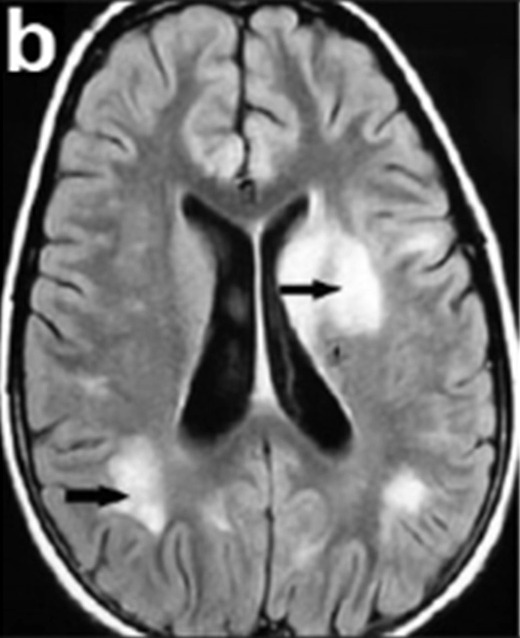
00:02 Our topic here is Acute Disseminated Encephalomyelitis. 00:06 So what does this mean to you? If you take a look at the picture here, it's a monophasic demyelinating disease that most commonly will be following a viral infection or a patient has received immunization. 00:19 That's important, it's got acute disseminated encephalomyelitis. 00:24 Please look for viral infection, and then following which may result in edema leading disease. 00:31 Symptoms develop a week or two after the antecedent infection. 00:35 Diffuse brain involvement: headache, lethargy, coma, in some cases. 00:41 Prognosis: Well, hear, recovery typically near complete. 00:46 For the most part, this particular issue goes away, as long as you're able to properly provide the supportive therapy for the viral infection, and immunomodulatory therapy with high dose methylprednisolone. 01:01 Like, less than 1/3 however, will go onto multiple sclerosis in the future. 01:04 So keep that in mind as well. 01:06 They want to think of this as being perhaps something like pre multiple sclerosis, if that helps you. 01:11 This was important pay attention to ADE viral infection. 01:19 This is transverse myelitis. 01:21 I'll give you one clinical pearl. 01:24 Stay away from the brain in this condition, okay. 01:28 The reason I say that if you say myelo, you'll notice there's no encephalo. 01:32 In addition, take a look at the schematic here. 01:36 There's no brain pictured here on purpose. 01:39 So, it's a demyelinating event restricted to the spinal cord. 01:43 Way back when, when we talked about spinal cord pathology or when you have reviewed it. 01:49 We talked about transverse myelitis as being the possible cause of trauma to the spinal cord. 01:54 Here you have it. 01:55 There is no evidence of brain lesion that is the absolute clinical pro that you want to take out of this. 02:01 Can be in isolation or associated with autoimmune disorders such as Sjögren. 02:06 Treated with steroids and plasmapheresis. 02:09 Why? Because you're thinking about autoimmune diseases, and can be recurrent is called transverse myelitis. 02:16 Look for autoimmune diseases for the most part, inflammation of the spinal cord with no involvement of the brain. 02:27 Our next topic, your patient comes in and well, was taking carbamazepine. 02:33 Why? Or to treat perhaps trigeminal neuralgia. 02:37 As a side effect, we get labs. 02:40 And under labs it shows that your sodium levels. 02:41 Sodium levels is 125. 02:44 Would you please put together? Carbamazepine a sodium level, that is what? Decreased, hyponatremia. 02:52 That your patient is coming in with hyponatremia. 02:54 You want to correct this. You want to correct this. 02:57 Unbeknownst to the resident, unbeknownst to the intern, Get all anxious, and extremely happy, and we wanted to correct this, and so therefore, to rapidly corrects the hyponatremia. 03:10 And in the process results in a condition called central pontine myelinolysis. 03:19 What's happening? Allowed the name to speak to you. 03:22 The pons, you're in the brainstem. 03:24 What's happening in the central portion of the pons, if you take a look at the picture here, it clearly tells you what's happening. 03:31 The lesion is in the central portion, the pons. 03:32 What's happening? Demyelination. 03:35 Why? Well, there are many theories out there. 03:37 At this point, what you're correcting for, too rapidly was the hyponatremia. 03:43 So what was there trying to say with carbamazepine? Carbamazepine causes a side effect of SIADH, syndrome of inappropriate antidiuretic hormone. 03:53 With too much ADH, what then happens your sodium levels? Hyponatremia. 03:58 And if you want to correct it too quickly, there's every possibility that the patient may suffer from central pontine myelinolysis. 04:05 That’s unfortunate. 04:05 This whole thing could have been prevented. 04:08 And really, the next step of management was to take the patient off the carbamazepine. 04:13 In this particular case, it could be also seen with alcoholics. 04:17 Anything that causes hyponatremia, and there's rapid correction. 04:21 It is the basis pontus classically, but could be other sites as well. 04:25 Keep that in mind. 04:26 Never, never correct your hyponatremia to rapidly. 04:30 Present with look at this, look at manifestations, it's devastating. 04:35 It's tetraplegia, quadriplegia. 04:37 The patient loses all ability to move. 04:41 I'm locked in. Isn't that a horrible feeling? You have all your limbs, you're completely aware, but yet, you can't move anything. 04:49 Could you imagine how the patient is going to feel? Because not you, but someone that you know, rapidly corrected the hyponatremia. 05:00 Common presentation: What you're going to find? Acute paralysis. 05:05 Maybe dysarthria, difficulty with speaking and dysphagia, you're knocked out the brainstem. 05:10 Holy cow, no joke. What happened? Don't correct the serum sodium to more than 10 units per 24 hours. 05:17 Clear? Memorize that. 05:19 Memorize that, and only then are you permitted to move on.
About the Lecture
The lecture Acute Disseminated Encephalomyelitis, Transverse Myelitis and Central Pontine Myelinolysis by Carlo Raj, MD is from the course Multiple Sclerosis. It contains the following chapters:
- Acute Disseminated Encephalomyelitis
- Central Pontine Myelinolysis
Included Quiz Questions
Which of the following autoimmune diseases is associated with transverse myelitis?
- Sjögren syndrome
- Rheumatoid arthritis
- Systemic lupus erythematosus
- Scleroderma
- Wegener granulomatosis
A 21-year-old man presents to your office with a runny nose, headache, and fever for the past three days. A viral infection is suspected. The patient feels better after symptomatic management, but soon after, he progresses into a lethargic state. Which of the following is correct in regard to his condition?
- Acute disseminated encephalomyelitis that typically has a good prognosis
- Acute disseminated encephalomyelitis with more than one-third progressing to multiple sclerosis
- Acute disseminated encephalomyelitis that involves the brain stem only
- Acute disseminated encephalomyelitis that involves the spinal cord only
- Acute disseminated encephalomyelitis that follows a bacterial infection
A 45-year-old Caucasian man presents to your office for his medication refill. He is on amlodipine, metformin, carbamazepine, and cimetidine. His medications are renewed, but soon after that visit, he is brought to the ER with a headache and confusion. What is the likely cause of his condition and the most appropriate step in the management?
- Hyponatremia and serum sodium correction not exceeding 10 mmol/L over 24 hours
- Hyponatremia and serum sodium correction not exceeding 10 mmol/L over 12 hours
- Hyponatremia and serum sodium correction not exceeding 5 mmol/L over 24 hours
- Hypernatremia and serum sodium correction not exceeding 10 mmol/L over 24 hours
- Hypernatremia and serum sodium correction not exceeding 5 mmol/L over 24 hours
Author of lecture Acute Disseminated Encephalomyelitis, Transverse Myelitis and Central Pontine Myelinolysis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
3 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Dr. Raj’s lectures have been very helpful to me in understanding complex concepts. Thank you
Dr. Raj nails it, easy and quick, to the point, nothing unnecessary, thank you!!!
this lecture is great, good level of detail and well explained!
