Playlist
Show Playlist
Hide Playlist
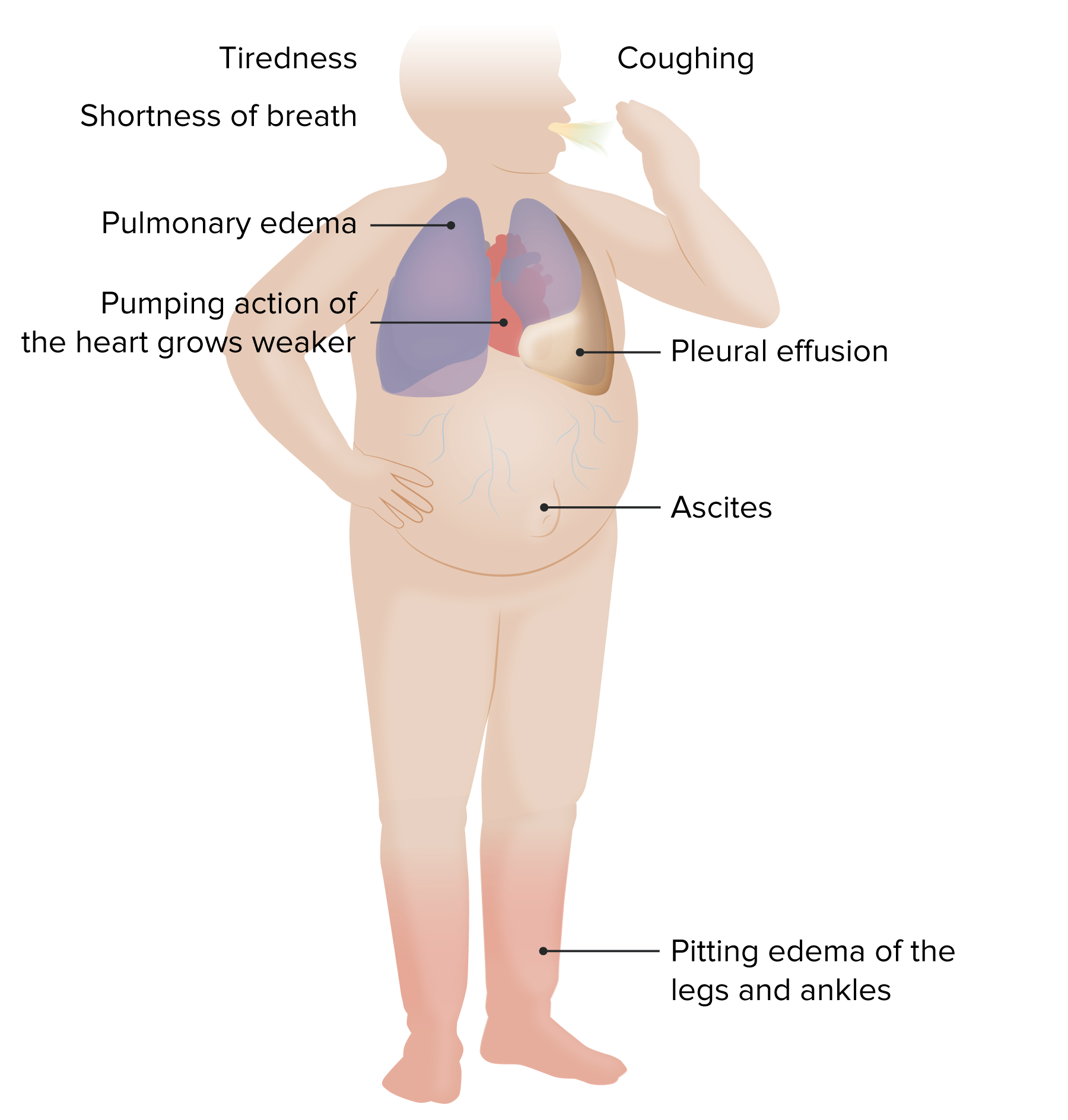
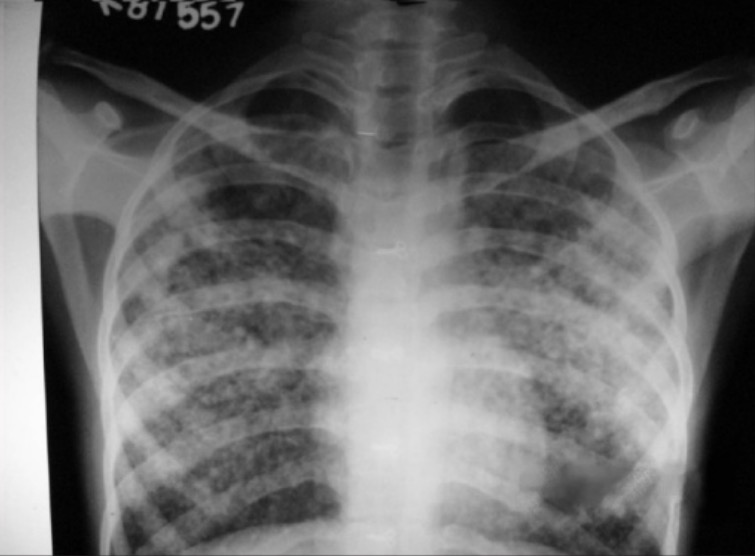
Acute Pulmonary Edema (APE): Management

-
Emergency Medicine Bord Pulmonary edema and CHF.pdf
-
Download Lecture Overview
00:01 You know, due to the presenting acuity of these patients, often times we treat and evaluate simultaneously. 00:07 So this is the patient who you’re gonna wanna try and get the history from. 00:10 The history might need to be obtained from the medical record, from the paramedics, from a family member. 00:16 And while you’re doing all that and you’re listening to the patient’s lungs and you may hear rales and crackles on the lung exam, you’re also gonna wanna be treating the patient so all of this is happening at the same time. 00:29 Often times, the medics will pickup these patients and they’ll start them on noninvasive positive pressure ventilation. 00:35 So this is either continuous positive airway pressure or bilevel positive airway pressure and what that does is that again helps to recruit more lung tissue. 00:44 The other thing that it does is it creates positive pressure in the lungs when the patient inhales and what that does is it helps expand the alveoli and the alveoli are necessary for air exchange. 00:57 So when you expand the alveoli and the fluid leaves the alveoli and goes back into the capillaries, that patient is gonna have decrease in their shortness of breath. 01:07 Now, noninvasive positive pressure ventilation has uses increased greatly over the last 10-15 years, and has really decreased the amount of intubations that we have to had to perform for these patients. 01:21 Sometimes, the paramedics will put these patients on CPAP before they get to the emergency department and by the time they get in they’re gonna look wonderful, they’re gonna look great, they’re gonna be very turned around within that short period of time. 01:33 Like I mentioned initially, these patients can turn around very, very, quickly. 01:37 Nitrates are the next thing that you wanna be thinking about and reaching for. 01:42 So nitrates are like nitroglycerin, is the main one that we use. 01:47 Nitroglycerin comes in a couple of different dosage forms. 01:50 So one of it is that you can do sublingual nitroglycerin and that’s the pill that’s also sometimes used if your patient is complaining of chest pain. 01:57 You can put that underneath the patient’s tongue. 02:00 The other form of nitroglycerin that can be given is given generally when a patient arrives in the emergency department and that’s IV nitroglycerin. 02:09 This is one of the situations where you’re gonna open up your Epocrates or whatever dosage app you have on your phone and it’s gonna tell you to start out with a very low dose. 02:19 In this situation, when someone has flash pulmonary edema, often times what we like to do is we like to start out in a higher dose to somewhere along lines of 400 micrograms a minute and as the patient gets better and gets the treatment, that medication can be titrated down. 02:34 Now nitrates can lower the blood pressure significantly and often times these patients have very elevated blood pressures so nitrates can help dilate the blood vessels and improve breathing and also can help with blood pressure lowering as well. 02:49 The other form of nitrates for a less critically ill patient would be nitrates that you can put on the skin that’s commonly known as nitro paste. 02:59 So you put it on a little card and the patient puts that on their skin. 03:02 Be careful if you’re doing that not to get any on your skin because it could potentially drop your blood pressure and make you pass out. 03:09 The diuretics are the last piece of the puzzle here. 03:13 Now, I wanna stress that you wanna do these other things first so you wanna do your noninvasive ventilation, you wanna do your nitrates and then you wanna be thinking about your diuretics. 03:22 Now, the reason for this is because those other two treatments take place very, very quickly and you will see effects very quickly from those treatments. 03:31 For diuresis, it does take a little bit more time to take effect. 03:34 When you’re dong diuresis for the most part you’re gonna be reaching for Furosemide first and when you’re reaching for that medication you wanna start out with a higher dose so you wanna start out, generally, with between 40 to 80 milligrams of Furosemide. 03:48 Again, it’s gonna take a little bit of time to work, but you wanna get it on board after he gets those other medications within the patient or you get the other treatments for the patient.
About the Lecture
The lecture Acute Pulmonary Edema (APE): Management by Sharon Bord, MD is from the course Respiratory Emergencies.
Included Quiz Questions
Which of the following is the main reason why diuretics are the last to be considered in the immediate management of acute pulmonary edema and CHF?
- They are too slow to act.
- Many patients are allergic to diuretics.
- Non-invasive positive pressure ventilation and nitrates should be administered first.
- They disturb the normal electrolyte balance in plasma.
- Patients must be observed closely upon administration.
Which of the following is NOT a treatment for acute pulmonary edema?
- Epinephrine
- Oral nitroglycerin
- Furosemide
- CPAP
- Nitropaste
Author of lecture Acute Pulmonary Edema (APE): Management

Sharon Bord, MD
Customer reviews
3,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
Very good thanks for the explanations, very clear oooo oooo oooo
feel confused from explnation,i need to repeat many times hope you change the video
