Playlist
Show Playlist
Hide Playlist
X-linked Dystrophinopathies and Duchenne Muscular Dystrophy

-
Slides Proximal Predominant Muscular Dystrophies.pdf
-
Download Lecture Overview
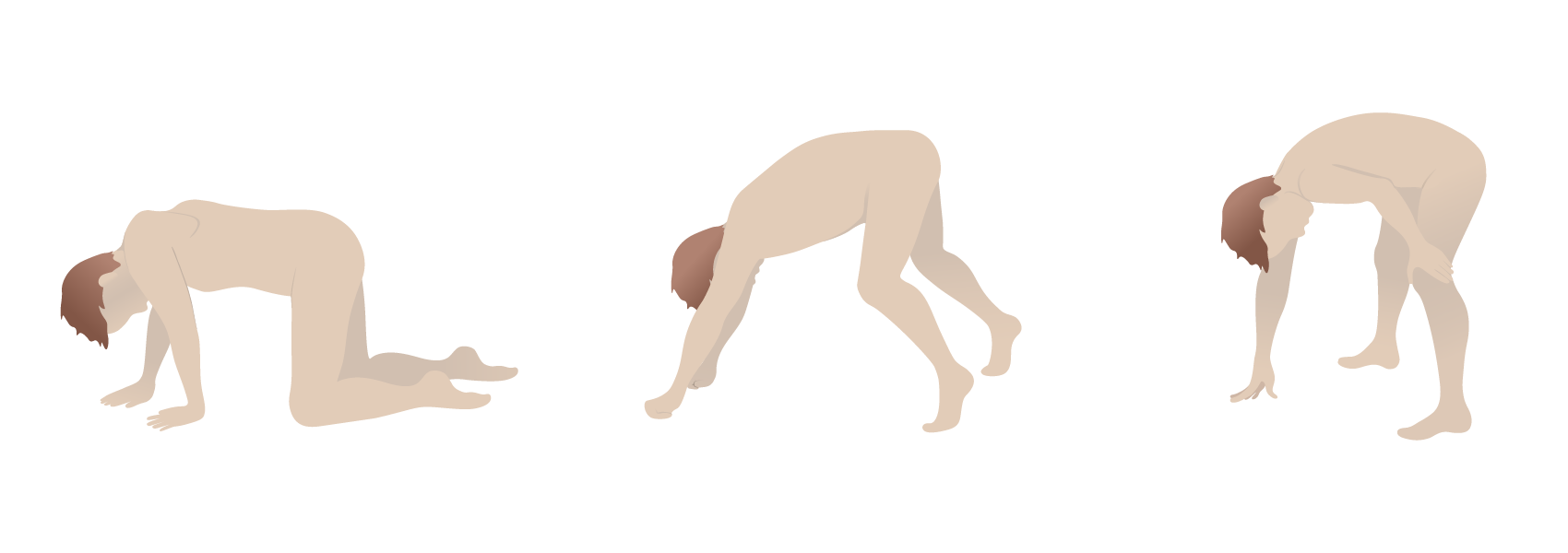
00:01 So let's think a little bit more about these dystrophinopathies. 00:04 And we're going to start with the x-linked dystrophinopathies. 00:08 And then we'll move to other inherited causes of muscular dystrophy, particularly limb-girdle muscular dystrophy. 00:14 There are two x-linked inherited muscular dystrophies and they are Becker's and Duchenne's muscular dystrophy. 00:21 We see these in young boys, who present with proximal weakness, and a prominently elevated CK. 00:28 And those three findings should really point us in the direction of thinking of Duchenne's and Becker's muscular dystrophy. 00:35 What's the distribution? We can see here in this schematic that this is a proximal predominant muscular dystrophy. 00:41 So, patients present with prominent leg and arm proximal weakness, difficulty with walking and running, and walking upstairs or running upstairs, getting up out of a chair, reaching up to high counters or cabinets, or those sorts of things to pull themselves up. 00:57 And in the severe cases, we can see Gowers's sign, where patients use their arms to walk themselves up from a seated position because of prominent proximal lower extremity weakness. 01:09 This distribution is really key to understand and to evaluate on exam. 01:16 What about the etiology? Let's start with Duchenne's Muscular Dystrophy and think a little bit more about the typical features there. 01:22 This is an X-linked recessive disorder that results from nonexistent or absent dystrophin. 01:29 And we'll think a little bit more about dystrophin the pathophysiology of Duchenne's Muscular Dystrophy and the subsequent slide. 01:36 This affects boys. 01:37 It is an X-linked muscular dystrophy, and though moms and women can be slightly affected, prominent presentations are in young boys. 01:48 So one of the typical manifestations of Duchenne's Muscular Dystrophy, we typically see weakness that begins, usually in the ages of two to three years is when the symptoms begin. 01:59 Patients present with early proximal muscle weakness, difficulty with jumping, and running, and walking, and getting up out of chairs. 02:07 And then calf pseudohypertrophy. 02:10 And this results from replacement of muscle with fibrosis, that increases the total volume of the muscle. 02:16 Even though the muscles are weak because of loss of muscle function. 02:20 the calf are hypertrophied. And this is a prominent finding. 02:23 It's something that's easily seen on exam to the astute eye, and points us in the direction of Duchenne's or Becker's muscular dystrophy. 02:31 What about the workup? What do we do to evaluate these young boys that present with proximal muscle weakness, and calf pseudohypertrophy? Well, the most important test is the CK. 02:41 And whenever we're evaluating any muscle disorder, we know that a CK is an important test and points us towards inflammation in the muscle. 02:49 And the CK is prominently elevated more than 10,000 times the upper limit of normal in most patients with Duchenne's muscular dystrophy. 02:58 Genetic testing is the next step. And this confirms the diagnosis. 03:01 This is a genetic or inherited cause of muscle weakness and muscular dystrophy. 03:07 What about the typical course? We use prednisone to treat these patients. 03:11 The inflammation in and around the muscle is the earliest, earliest finding and is treated with prednisone or anti inflammatory. 03:19 That early inflammation leads to subsequent degeneration and necrosis of the muscle. 03:24 And so in late stages, prednisone is not helpful. 03:26 And this is a treatment that we really begin early in the course of therapy to prevent prominent respiratory weakness, early in the course of the disease. 03:36 Patients do ultimately die of this disease frequently, and that's often from respiratory muscle weakness, and typically pneumonia. 03:43 What's the prognosis? Men have a shortened lifespan. 03:47 They often live into the third or fourth decades of life. 03:51 And there are new treatments that are being explored. 03:53 And we'll discuss those in some of the next slide. 03:55 I think importantly, sometimes we diagnose a young boy with this condition and find that mom also has symptoms that have gone unrecognized. 04:03 And this may present with mild weakness or cardiac conduction abnormalities, that can be a tip off to this inherited predisposition. 04:13 So what are some of the treatments? What are some of the other treatments that we would consider for Duchenne's Muscular Dystrophy? Well, there's really three that I want you to know. 04:20 The first is prednisone. This is a tried and true treatment. 04:24 This is something that we've been utilizing for decades for these patients. 04:27 And it's best when initiated early. 04:29 It's been used the longest. 04:31 It reduces muscle inflammation, which is seen early in the condition and results in that elevation of CK. 04:38 And it's effective early. 04:39 And so it's really a treatment that we begin early when evaluating and diagnosing these patients. 04:44 The second and a more recent treatment to come onto the market is deflazacort. 04:49 It is a similar medication and acts very similar to prednisone. 04:53 It's a glucocorticoid and so it has a similar mechanism of action. 04:57 Its potency is around 70% to 80% that of prednisone. 05:01 But it costs a lot of money around 80,000 per year. 05:05 And so in clinical practice, we often see prednisone being favored over deflazacort, except in those patients who may not respond to prednisone. 05:13 And then the last treatment that I'd like for you to know, and perhaps the most interesting these days is Exondys 51. 05:21 This acts very differently to prednisone and deflazacort. 05:24 It is an antisense oligonucleotide, and it really works as an exon skipping agent, which we'll talk about in the next slide. 05:33 It works as a bridging piece of DNA or RNA so that the dystrophin protein can be made. 05:41 It only works for specific Duchenne's Muscular Dystrophy mutations, and we'll talk about some of those. 05:48 And the thing to remember with this medication is it is an exon skipping therapy, really unique mechanism of action. 05:55 So how does it work? What's happening with Exondys 51? Well, here we see what happens in the healthy adult or healthy child. 06:04 Duchenne's muscular dystrophy, pre-mRNA is composed of a number of exons, and that's exon 48 to 49, 50, 51, 52. 06:14 In order to make a normal healthy dystrophin protein, those exons are spliced into a messenger RNA, and you can see the messenger RNA here contains exon 48, 49, 50, 51 52. That's really important. 06:29 And ultimately, that messenger RNA is translated into the functioning dystrophin protein. 06:34 And that's what happens in the healthy individual. 06:38 In Duchenne's muscular dystrophy, we see that a mutation results in an early stop code on and there is incomplete transcription and translation of that dystrophin protein. 06:50 So we see a fewer number of exon's. 06:52 Here exon 48 to 51, and 52 as a result of mutation in exon 49, or 50. 06:59 Results in a truncated or early premature stopped messenger RNA, and a lack of any dystrophin protein. 07:08 So what does Exondys 51 do? This is a antisense oligonucleotide that skips the coding of exon 51. 07:17 So instead of transcribing exon 51, we skip that and we see we are resulted with a messenger RNA containing exon 48 and 52. 07:27 And this is sufficient to generate a shortened but functional dystrophin protein. 07:32 Doesn't have all of the normal functions of dystrophin, but substantially improves the situation within the muscle and symptoms in these Duchenne's Muscular Dystrophy patients. 07:43 and exon skipping therapy.
About the Lecture
The lecture X-linked Dystrophinopathies and Duchenne Muscular Dystrophy by Roy Strowd, MD is from the course Hereditary Neuromuscular Disorders.
Included Quiz Questions
Which of the following patient characteristics is most suggestive of an X-linked muscular dystrophy?
- Young boy
- Middle-aged woman
- Distal muscle involvement
- Low CK levels
Which of the following clinical findings might suggest a diagnosis of Duchenne’s MD?
- Difficulty getting up from a seated position
- Average jumping and running capability for age
- Normal CK levels
- Calf muscle wasting
- Weakness developing in early adulthood
When discussing the prognosis of Duchenne’s MD with a new patient, which of the following statements is most accurate?
- Respiratory muscle involvement results in pneumonia and ultimately death.
- Patients with this disease will live largely normal lives until late adulthood.
- Gender does not impact life expectancy from this disease
- There are therapeutic options at this time.
- Once diagnosed, the patient’s symptoms are likely to improve with time.
Which of the following statements concerning eteplirsen is most accurate?
- It acts as a bridging oligonucleotide, allowing some dystrophin to be synthesized by the patient.
- The treatment has equal efficacy for all patients with Duchenne’s MD.
- The drug is a synthetic version of physiologic dystrophin.
- The mechanism is considered intron-skipping therapy.
- This treatment is curative for most patients.
Author of lecture X-linked Dystrophinopathies and Duchenne Muscular Dystrophy

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
