Playlist
Show Playlist
Hide Playlist
Vitamin B9 (Folic Acid)

-
Slides WaterSolubleVitaminsII Nutrition.pdf
-
Download Lecture Overview
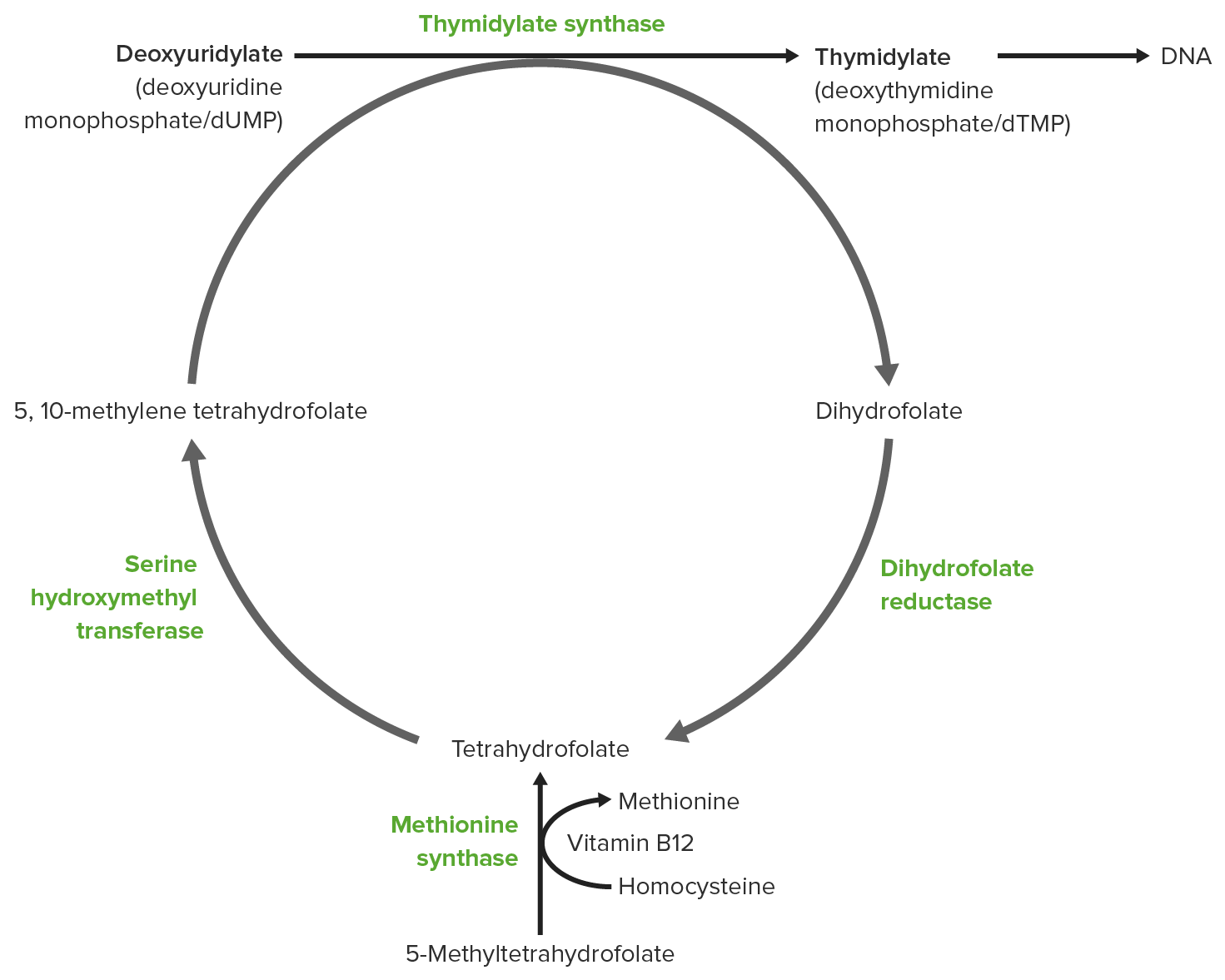
00:00 So here in our second lecture on water soluble vitamins, we'll be addressing B9 and B12 which are pretty tightly tied together as well as vitamin C. 00:13 Which is a little bit more simple after we get through these. 00:17 So B9 is folic acid or folate. 00:21 And B9 is primarily involved or it's biggest feature is that, it's involved in nucleotide production. 00:29 So anytime we need more DNA, we need to have a lot of folate. 00:36 That's also involved in methylation of DNA. 00:40 So again, anytime we have extra cell division going on, we need additional folate. 00:47 So, imagine sometimes if you can where we might see extra cell division going on. 00:54 Of course we know that we have uncontrolled cell division in cancer. 00:59 And everytime there is a cell division each new cell needs a new copy of DNA. 01:03 And thus the demand for nucleotides goes up. 01:07 Pregnancy of course is a time where we have increase cell divsion. 01:12 So it's very important for a pregnant patient to make sure they are taking in enough folic acid. 01:19 During infancy a child is going under loads of cell divisions to grow. 01:24 And finally hemolytic anemias like sickle cell anemia. 01:29 We definitely need to have more DNA because these bloods cells are being destroyed. 01:34 And we have an increased rate of cell division in the blood cells. 01:37 And they need their own DNA. 01:39 And so folate demands go up. 01:43 So anytime we have exta cell division, we may have a deficiency in folic acid. 01:49 And that will present itself as megaloblastic anemia. 01:54 Now what happens in megaloblastic anemia. 01:56 Mega is sort of the key there. 01:59 With megaloblastic anemia we see that there is a decreased red blood cell count or decreased hematocrit, right. 02:09 And this is because cells are not making it pass that G1S checkpoint. 02:16 So the cells grow. 02:18 Their checkpoint to see if their DNA is ready to go on and be synthesized in S-phase isn't passed because the cell doesn't have enough nucleotides due to a folate deficiency. 02:32 And so the cell will continue to grow. 02:36 So we have an increase in cell volume. 02:40 And thus, we call them macrocytic cells. 02:43 You can see the ones on the left here have much more cytoplasm in them versus the normal ones on the right. 02:50 Normoblasts in the presence of enough B12 are the right size, right distribution of cytoplasm. 02:59 So, when we consider folate, we really need to dig into the metabolism. 03:06 So I haven't really highlighted any of the particular or specific pathways that the vitamins have been involved in so far. 03:15 But this one is an important one for you to get a handle on. 03:18 You'll notice that the last slide said that we had an increase in homocysteine. 03:25 Now, what is that have to do with anything you might ask. 03:29 And that's where we need to take a step into the pathway involved. 03:34 Because it also has to do with B12. 03:37 As I said they are very tightly tied together. 03:40 So first of all over here, we have the intake of folate. 03:45 And then the whole bunch of other steps along the way. 03:48 You probably are familiar with some of these intermediaries already. 03:54 But if you're not, don't panic. 03:55 Let me assure you that the whole point here is, we have folate intake and it is going to end up in DNA synthesis if we have plenty of folate present. 04:07 If there is not enough folate present, this pathway gets shutdown. 04:10 And we see that there are the problems of megaloblastic anemia. 04:15 So let's go back to the details, don't panic. 04:18 First we have folate. 04:21 And folate gets turned into dihydrofolate and tetrahydrofolate. 04:25 And then mythelenetetrahydrofolate and methyltetrahydrofolate. 04:32 So what's the big story here. 04:35 As I mentioned before we end up from this tetrahydrofolate getting some precursors for DNA. 04:43 Those are one pathway, one option we can create some amino acids, some purine synthesis but the piece where we're going to tie B9 and B12 together, is right here. 04:56 Because methyltetrahydrofolate cannot do anything functional as far as DNA production. 05:05 Cannot be used as a precursor for any nucleic acids or purines or pyrimidines for that matter. 05:12 We have a recycling program where mythelenetetrahydrofolate is actually recycled and converted back into dihydrofolate by an outside pathway. 05:24 While at the same time creating nucleic acids which can lead to more DNA production. 05:30 So everybody's happy and that's excellent. 05:33 But how do we get this recycling to continue and where does homocysteine come in. 05:41 So when we have methyltetrahydrofolate it is not going to be recycled to tetrahydrofolate unless B12 is present. 05:54 Because we have to get rid of that methyl group. 05:56 Tetrahydrofolate doesn't want it. 05:58 B12 comes along, snags it. 06:01 Takes it away for a moment and now B12 has the methyl group. 06:06 And it doesn't want it either so it passes it right on to homocysteine and causes the production of methionine. 06:15 Now if we don't have enough folate this pathway slows down. 06:19 And we see that there is a build up of homocysteine. 06:23 Clearly you can see that B12 deficiency could result in this build up also. 06:30 So this is a pathway that you should be familiar with as you go into your exams and we will revisit it in some details here again shortly. 06:42 So very few pathways that I've really pushed. 06:44 This one's one that you should certainly get a grip on. 06:48 Before we move on from folate or folic acid, I wanted to remind you of a couple of drugs that have an impact on it. 06:57 Trimethoprim is an antibiotic. 07:00 And methotrexate is a drug that's commonly used in chemotherapies. 07:05 And both of these drugs inhibit folate production. 07:10 So patients that are taking either of these drugs should be supplemented with additional vitamin B9 or folic acid.
About the Lecture
The lecture Vitamin B9 (Folic Acid) by Georgina Cornwall, PhD is from the course Nutrition. It contains the following chapters:
- Vitamin B9 - Folate (Folic Acid)
- Folate Metabolism
Included Quiz Questions
A person is undergoing chemotherapy with methotrexate. Their complete blood profile revealed decreased red cell count, decreased hematocrit, and raised MCV. They also have high levels of homocysteine. Which of the following vitamins is most likely deficient?
- B9
- B1
- B2
- B3
- D
In which of the following processes is vitamin B9 is involved?
- Nucleotide production
- Synthesis of heme
- Synthesis of dopamine
- Carboxylation reactions
- Oxidation of fatty acids
Which vitamin is given to pregnant women to prevent neural tube defects in the developing fetus?
- Folic acid
- Pyridoxine
- Pantothenic acid
- Niacin
- Biotin
Which vitamin B9 metabolite is needed for the conversion of homocysteine to methionine?
- Methyltetrahydrofolate
- Methylenetetrahydrofolate
- Tetrahydrofolate
- Dihydrofolate
- Vitamin B12
Author of lecture Vitamin B9 (Folic Acid)

Georgina Cornwall, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
