Playlist
Show Playlist
Hide Playlist
Sequence of Depolarization – Electrocardiogram



-
Slides CV Physiology-Electrocardiogram.pdf
-
Download Lecture Overview
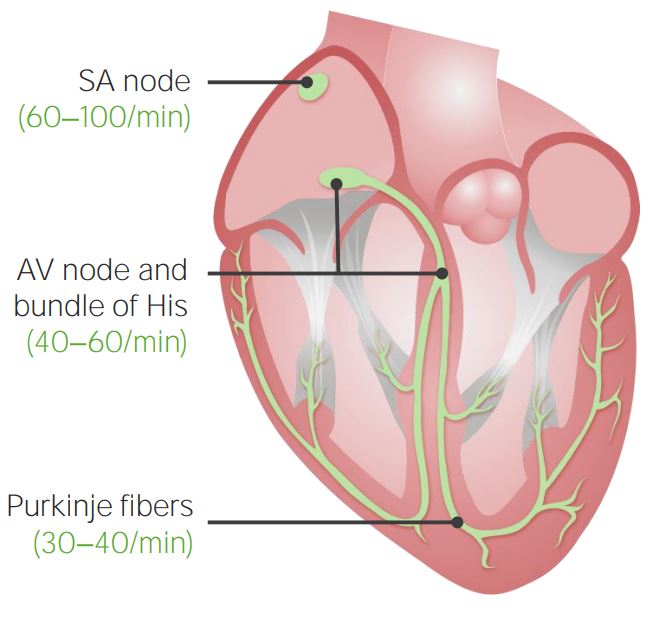
00:01 So, let's trace through now the standard ECG and how that links up with the spread of depolarization throughout the heart. 00:11 So, where do we start? We start at the primary pacemaker – the sinoatrial node. 00:17 The SA node is our starting point. 00:20 Here, you have a depolarization that occurs, and that forms a wave that we call a P wave. 00:29 You have a little bit of a delay that happens and that delay occurs in the AV node. 00:39 The QRS complex is a little bit more complex. 00:42 So, let's talk through that in step-by-step form. 00:48 The first portion of the QRS complex is a small downward deflection. 00:55 This small downward deflection is because the septum of the heart depolarizes from the left to the right. 01:05 Now, this is kind of hard to think about. 01:08 Why would a depolarization moving from the left to the right cause a small negative deflection on the ECG? Remember that it's all about the mean electrical or the mean axis of this particular depolarization. 01:26 That can be seen here as a small travel towards the negative pole, so if a negative deflection is a small positive force traveling towards the negative pole. 01:45 That’s hard for a second. 01:47 Let’s step through the other three examples and come back to this one because we started with the hardest one. 01:53 Let’s go to the next one. 01:56 We have a positive deflection as you have depolarization going to the apex of the heart. 02:04 This makes a lot more sense, right? You have a large vector traveling towards the positive pole. 02:11 If you had traveling towards the positive pole, what do you get? A positive deflection. 02:17 Okay? Now, as you continue to de-polarize the ventricle, especially the left ventricle, it starts to travel down towards baseline. 02:28 And once it's completely depolarized, you’re back down to baseline levels. 02:34 So, let’s revisit number one again, right? Because that was hard. 02:38 Why did we get a small negative deflection when the septum of the heart depolarized from the left side to the right side? Here, because that mean vector traveled a little bit towards the negative pole. 02:55 A positive deflection traveling towards a negative pole is a negative deflection on the ECG. 03:02 If you have a positive charge traveling toward the positive pole, it is a positive deflection on the ECG. 03:12 So, the other item that we need to bring out is why did we have the electrical signal that's traveling towards a positive pole, it was heading up right, and then as you went to the next form, it started to head back down again. 03:26 Let's explain that in more detail. 03:29 So, we start off with a normal ECG recording. 03:33 It's a flat line. We call that isoelectric. 03:38 If you can imagine this point A on this graph as being a negative electrode and let's say B is a positive electrode, when you’re at electrode neutral, you have a flat line. 03:54 As a depolarization starts and heads towards a positive pole, you get a positive deflection, right? Positive traveling towards the positive pole, in this case is B, is a positive deflection. 04:09 You continue to travel towards that positive pole, it gets more deflected. 04:15 In fact, halfway to the point in which you're going to reach that positive pole is your maximal deflection. 04:24 Then – this is where it gets a little hard. 04:27 Follow me. Follow me. Here we go. 04:30 If you keep traveling past the halfway point, you still have a positive deflection, but it is a little bit less of a deflection than you had at the maximal point, which was halfway. 04:44 Then if you complete the depolarization process, it returns back to baseline. 04:50 All of it’s depolarized. 04:53 And then you're back to the isoelectric line. 04:56 So, this is how a positive depolarization traveling towards a positive pole causes both an upward deflection and then a return to isoelectric baseline. 05:10 But note that all of that is positive. 05:12 The whole wave is positive. 05:17 Okay. 05:18 So, now that we have a positive charge traveling towards a positive pole and giving us a positive deflection, let's talk more about the QRS complex. 05:29 The QRS complex can be divided into four. 05:32 One is the Q wave. 05:35 Two is the R wave as it's starting to peak. 05:38 Three is the return of the R wave. 05:41 And four is a little bit of a negative deflection. 05:46 So, one through four. 05:49 This is the ventricular depolarization process. 05:53 It’s called the QRS complex. 05:55 It has a certain duration. 05:58 It's going to be somewhere in between 0.06 and 0.1 seconds. 06:06 It's very much related to the mass of the tissue. 06:10 The bigger the mass, the more the deflection. 06:14 And smaller the mass, the less the deflection. 06:19 What you want to think about here is the more tissue that it has to move through, the greater that electrical activity. 06:28 More tissue, more electrical activity. 06:32 If you really think about this, it makes sense. 06:35 If someone has left ventricular hypertrophy, you have more tissue and, therefore, it's going to show up as larger amplitudes on your various waveforms. 06:45 The other thing that’s very important to think about for the QRS complex is where your electrodes are. 06:51 Now, we went through this earlier on that you can take multiple pictures of the heart, right? So, it very much depends where your positive electrode is and where your negative electrode is to know what this picture is going to look like. 07:06 Because we’re simply following these vectors. 07:10 So, if you match the positive pole right to where that vector is, you're going to get the greatest deflection. 07:17 If you change up where the poles are, you can get a totally different looking ECG, even though the heart hadn't changed, you just re-oriented where you're taking the picture from. 07:31 So, the most important thing to think about is where the mean electrical axis is in this response, and that is going to tell you where the most positive deflection will be if you arrange the electrodes in that format, where the positive pole is right at the mean electrical axis.
About the Lecture
The lecture Sequence of Depolarization – Electrocardiogram by Thad Wilson, PhD is from the course Cardiac Physiology.
Included Quiz Questions
Which of the following likely causes the small downward deflection in the QRS complex of the ECG?
- Septal depolarization
- Right atrial depolarization
- Apex depolarization
- Base depolarization
- Left atrial depolarization
Which direction will the ECG deflect when a depolarization travels toward a negative electrode?
- Downward
- Upward
- No deflection
- Inward
- Outward
Which of the following corresponds to the QRS complex?
- Ventricular depolarization
- Atrial repolarization
- Right ventricular repolarization
- Left ventricular repolarization
- Atrial depolarization
Author of lecture Sequence of Depolarization – Electrocardiogram

Thad Wilson, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
