Playlist
Show Playlist
Hide Playlist
Vascular Disease: Diagnosis and Treatment – AKI

-
Slides Nephrology Acute Kidney Injury.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
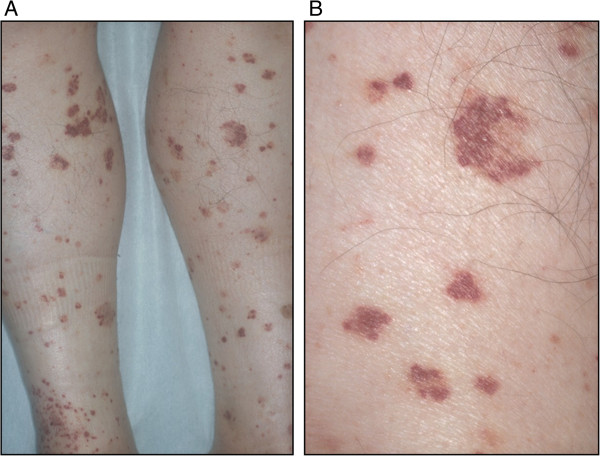
00:01 So when it comes to vascular diseases, how are we gonna clinch that diagnosis and figure out what's going on with our patients? Just as we've said with every single portion of this lecture, it's very important to be a diligent detective and really do a thorough history and chart review. 00:18 So, it's gonna be important to look in our chart or ask our question to our patients, 'have you had any kind of aortic manipulation within the past 2 to 8 weeks? If so, we're really thinking about cholesterol emboli. 00:30 How about a patient coming in with mental status changes and neurological abnormalities? or a history of having a diarrheal prodrome? If that’s the case, I'm really gonna be thinking more about thrombotic microangiopathies like TTP or HUS. 00:44 And how about a patient who's coming in with malignant hypertension, uncontrolled hypertension with blood pressures as high as 180/120. 00:53 I'm really going to be thinking about a renal associated TMA for malignant hypertension. 00:58 Physical exam can also be very helpful for us when it comes to diagnosing our patients. 01:03 So somebody coming in with cholesterol emboli may have things like livedo reticularis again as seen in this photo here. 01:11 They could also have something called blue toe syndrome. 01:15 So sometimes, when you're doing aortic manipulation or manipulation of any of those large arteries, you can have a massive amount of cholesterol emboli that will embolize distally and it can actually cause ischemia to the entire extremity as seen here With thrombotic microangiopathies, our patients oftentimes can manifest with purpura and petechiae, and that makes sense because they have thrombocytopenia And of course, with malignant hypertension, our patient will be coming in with very high blood pressures, typically with end-organ damage and blood pressures greater than 180/120 Laboratory evaluation is also important. 01:57 In cholesterol emboli syndrome, we can see things like low complements because complement is activated. 02:02 We have recruitment of inflammatory cells into those vessels where the ischemia is happening. 02:08 We can also if we have the right time, we can see that peripheral eosinophilia which can be very helpful. 02:14 And then when we look at the urine analysis, it's typically bland but if we're lucky enough, we can actually see a cholesterol crystal in there as well. 02:22 Again, I want to underscore the importance here because looking at that urine, if I don't see muddy brown cast as I would see in ATN, this is very helpful again to distinguish between the entity of radiocontrast exposure from ATN and renal atheroembolic disease from cholesterol emboli. 02:41 So, for a laboratory evaluation forTMA, we can see things like thrombocytopenia - low platelets. 02:48 We can see schistocytes on the peripheral smear. 02:51 So remember what is happening, we have those platelet thrombi, we have problems with the red blood cells kind of going through in being lysed so you have intravascular hemolysis as shown here, and our urine analysis may have red blood cells. 03:05 So when it comes to treatment of our patients who has the TMAs, it's really gonna depend on the cause. 03:11 So for renal atheroembolic disease, or cholesterol emboli syndrome, it's unfortunate because we don't have a lot of therapies that can help to mitigate the response of what's going on other than just treating our patient supportively. 03:22 That means that what I want to do is I need to ensure that nothing else happens to that patient in order to progress their disease. 03:29 So I want to avoid things like nephrotoxic exposures and make sure my patient's blood pressure is controlled. 03:37 If my patient has vasculitis then I'm really going to target that underlying cause or condition And then treat them specifically with immune-mediated therapy that targets that particular condition. 03:50 For thrombotic microangiopathies again, it’s gonna be very dependent on the condition that's manifesting. 03:56 If my patient has TTP, I'm going to do plasma exchange where I can actually remove those autoantibodies that are affecting that ADAMTS13 activity so that von Willebrand factor can be cleaved. 04:12 For Shiga-toxin associated HUS, that's the one remember we talked about with the diarrheal prodrome. 04:18 Unfortunately there's nothing that we can do other than provide supportive care but that's gonna be critical in that population again to make sure that my patient has adequate volume status and make sure that they don't have nephrotoxic exposures. 04:30 For complement-mediated TMA, this is probably one of the most exciting topics If those patients do in fact have a genetic mutation or an autoantibody that they've acquired that again is causing this constitutive activity at c3 convertase, we actually have a therapy available now which is a monoclonal antibody to C5 and can actually prevent formation of that membrane attack complex. 04:53 So it's pretty exciting although I have to say, it's very costly. 04:57 And then finally for the drug induced TMA, we simply remove the offending agent or the offending drug.
About the Lecture
The lecture Vascular Disease: Diagnosis and Treatment – AKI by Amy Sussman, MD is from the course Acute Kidney Injury (AKI).
Included Quiz Questions
Which of the following is a sign of thrombotic microangiopathy?
- Petechiae
- Livedo reticularis
- Blood pressure > 180/120 mm Hg
- Blue toe syndrome
Which of the following may be seen on urine microscopy with cholesterol emboli-induced thrombotic angiopathy?
- Bland sediment
- Urate crystals
- Cellular casts
- Muddy brown casts
A patient presents with elevated creatinine and schistocytes on a peripheral blood smear. Thrombotic thrombocytopenic purpura is suspected. What is the most appropriate treatment option?
- Plasma exchange
- Supportive care
- Eculizumab
- Hydrocortisone
Author of lecture Vascular Disease: Diagnosis and Treatment – AKI

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
