Playlist
Show Playlist
Hide Playlist
Vascular Disease: Causes – AKI

-
Slides Nephrology Acute Kidney Injury.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
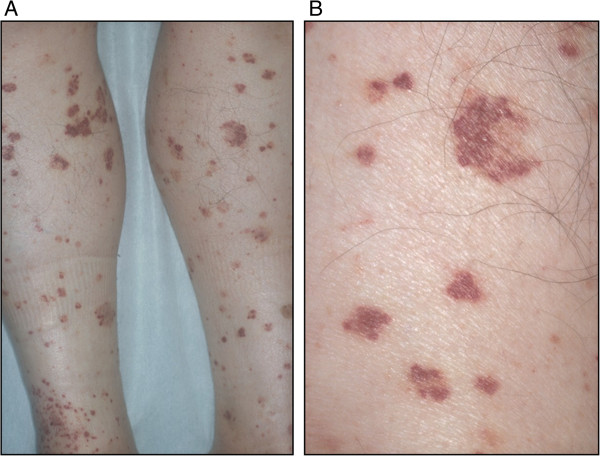
00:01 So we're now moving to our vascular diseases of the kidney. 00:04 And there's three main broad categories I want you to think about when it comes to vascular diseases. 00:09 The first is what we just talked about in our case, which is renal atheroembolic disease. 00:15 So this typically occurs in patients who have a very heavy atherosclerotic disease burden and anytime they undergo something that would involve manipulating the aorta, or any of the large arteries, they will be at risk for developing renal atheroembolic disease. 00:31 This includes things like coronary angiography just as in the case of our gentleman, and percutaneous coronary intervention, placing stents or doing the angioplasty to any of those coronary arteries. 00:42 It also is going to involve anything that will cause aortic manipulation so for example if I have a patient who's coming in and they have an aortic aneurysm and they're getting an endovascular aortic repair, then that can also cause that plaque burden to embolize distally. 00:58 Renal artery angioplasty and stent placement is probably the worst culprit when it comes to developing renal atheroembolic disease and you can think about why that would happen. 01:08 I've got my renal artery here, I've got a very heavy disease burden of atherosclerotic disease. 01:13 If I go in there and I try to angioplasty or place a stent, it's very easy for me to dislodge those pieces of cholesterol and have them embolize distally into those small arterioles in the kidney. 01:25 So again, just as what we've been talking about with each of these phenomena, cholesterol plaque can break off after that manipulation, it embolizes distally and it then leads to partial or total occlusion of multiple small arteries or glomerular arterioles. 01:41 So when that happens, what we typically see is that serum creatinine serologically that rise is gonna be more subacute. 01:48 It's happening over time because these pieces of cholesterol tend to just embolize a little bit at a time. 01:55 So we will tend to see this phenomena somewhere between 2-8 weeks following manipulation or procedure. 02:01 Again, let me go ahead and contrast this to what we've talked about before in our ATN section. 02:06 So when we give radiocontrast and our patients develop ATN from having radiocontrast, that's that iodinated contrast that causes tubular toxicity. 02:15 That rise in creatinine is really gonna be more at 72 hours at most. 02:20 So they tend to get that injury right within the first three days after contrast exposure. 02:25 When they have renal atheroembolic disease, even though they're getting contrast, that phenomena of those cholesterol emboli that are embolizing to those distal arterioles, that takes time for that to happen because once they embolize, they cause ischemia, they cause an inflammatory recruitment and that's really more subacute in that 2-8 week time frame. 02:47 I really want you to understand the difference between that because this is something clinically that you're going to see and you're gonna be able to better diagnose these two entities and you're also gonna see it in your licensure exam, so that's important. 03:00 So, the other thing with renal atheroembolic disease serologically is it's going to be associated with low complements in the serum just as we saw in the gentleman in the case. 03:09 They tend to also get an eosinophilia and a rash if we're lucky enough to see it just as you can see in this picture over here. 03:16 This is a rash that's representative of livedo reticularis. 03:22 Okay, so that's renal atheroembolic disease. 03:25 Let's move to our next category of vascular diseases, and that's vasculitis. 03:30 So vasculitis is inflammation and necrosis of small to medium-sized arteries and arterioles specifically in the kidney. 03:38 So this is going to include polyarteritis nodosa which has an association with hepatitis B, granulomatosis with polyangiitis formerly known as Wegener's granulomatosis, and then finally microscopic polyangiitis. 03:55 Now we're gonna talk about those latter two which is GPA and microscopic polyangiitis in our nephritic syndrome lecture. 04:01 And they are two of my favorite entities to discuss, so stay tuned for that. 04:06 Okay, our third broad category of vascular diseases, are the thrombotic microangiopathies or TMAs. 04:14 So what TMA refers to is any kind of injury to the endothelial lining of the blood vessel, then will result in platelet thrombi occluding those small vessels and causing ischemia. 04:28 The way that TMA manifest clinically is we will see thrombocytopenia, meaning that we've got low platelets, a microangiopathic hemolytic anemia, that means that we have intravascular hemolysis of these red blood cells in the circulation. 04:45 There's a couple of different entities that I want you to think about when it comes to TMA. 04:51 So the first of these is thrombotic thrombocytopenic purpura or TTP and this is characterized by a pentad of fever, neurological abnormalities, renal failure and of course thrombocytopenia and microangiopathic hemolytic anemia. 05:08 The next to think about is Shiga-toxin mediated hemolytic uremic syndrome. 05:13 This is associated with Shiga toxin-associated E. coli producing organisms, formerly known as diarrhea-associated HUS. 05:21 When we think about Shiga-toxin mediated HUS, those patients typically will present with the diarrheal prodrome. 05:29 The next is complement-mediated TMA, formerly called atypical HUS. 05:35 Complement-mediated TMA is very interesting because these patients tend to have genetic mutations in their complement system or acquired autoantibodies that cause constitutive activation of c3 convertase and formation of the membrane-attack complex. 05:51 The next to think about is drug-induced TMA. 05:54 So these are drugs like gemcytabine, lincomycin, calcineurin inhibitors. 05:59 Those drugs actually cause injury to the endothelial lining and that's what precipitates the TMA, again manifesting with microangiopathic hemolytic anemia and thrombocytopenia. 06:10 And finally our last category to think about when it comes to the TMAs is malignant hypertension. 06:16 So patients who manifest with very high blood pressures who typically have end-organ damage, will have a renal-limited TMA. 06:25 They may not always manifest with microangiopathic hemolytic anemia and thrombocytopenia, but certainly the pathological abnormalities are there on biopsy.
About the Lecture
The lecture Vascular Disease: Causes – AKI by Amy Sussman, MD is from the course Acute Kidney Injury (AKI).
Included Quiz Questions
Which of the following causes obstruction in atheroembolic renal disease?
- Cholesterol emboli
- Immunoglobulin light chain accumulation
- Radiocontrast exposure
- Blood clot emboli
Which of the following vasculitides is associated with hepatitis B?
- Polyarteritis nodosa
- Granulomatosis with polyangiitis
- Microscopic polyangiitis
- Giant cell arteritis
A young boy eats an undercooked hamburger at a barbecue and later develops diarrhea and bloody urine. Which of the following is most likely related to these symptoms?
- Shiga toxin-mediated hemolytic uremic syndrome
- Thrombotic thrombocytopenic purpura
- Complement-mediated thrombotic microangiopathy
- Enterotoxigenic Escherichia coli infection
Author of lecture Vascular Disease: Causes – AKI

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I did not know it was possible to teach so well as Dr. Sussman does. Even though nephrology is my least favorite part of internal medicine, it is so well explained that I actually enjoy learning it. This lecture, like all others, is so masterfully organized and explained that I can easily process the concepts and correlate them with everything else I have learned so far.
