Playlist
Show Playlist
Hide Playlist
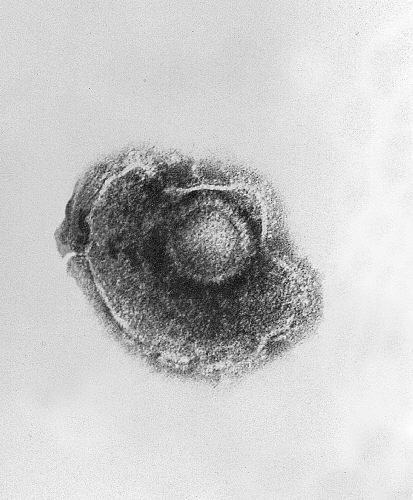
Varicella-Zoster Virus (VZV) – Herpesviruses

-
Slides Herpesviridae.pdf
-
Download Lecture Overview
00:01 Okay. 00:02 Let's move on to herpes number 3, varicella-zoster virus, the cause of chicken pox, and shingles. 00:09 Transmission of this virus, again, as with others, can be through respiratory, meaning sneezing, respiratory droplets, but also an especially close contact with active lesions. 00:21 Prevention for the varicella virus is via a very active vaccine. 00:27 It's live, but attenuated. 00:29 It's administered in childhood beginning at 12-15 months of life, and a booster is given at around age 4-5 years. 00:37 There now is a even higher potency zoster virus vaccine for adults to try and prevent the reactivation that we'll talk about very shortly. 00:47 Pathogenesis. 00:48 Initial infection with varicella-zoster virus also hits the mucoepithelial cells. 00:53 You see a recurring target here with the first 3 viruses, and then it is spread through the reticulo- endothelial system or bloodstream throughout the body. 01:02 So rather than being a focal target as we talked about with the first 2 herpes viruses, this one actually can spread throughout a viremia per sorts, and then any and all mucoepithelial cells throughout the body can be affected. 01:17 For the first several days, one develops flu-like symptoms as these virally-infected cells go through lysis. 01:23 And then we get chicken pox, the actual varicella related to reactivated or activation of the lytic lesions. 01:32 The latency with varicella-zoster virus is in the dorsal route or trigeminal ganglia, which is important when reactivation occurs causing shingles because that will occur in a specific dermatomal distribution of the trigeminal ganglia or the dorsal root nerve focus where the latency occurred. 01:53 So, let's compare and contrast the 2 diseases associated with varicella-zoster virus. 01:58 First, the incubation. 02:01 Chicken pox, during the incubation period is 3-7 days, during which time the patient may be asymptomatic. 02:09 But toward the end of that time, they'll develop typical viral, flu-like illness. 02:14 So, fever, some sore throat, a cough, "Oh, I think I'm coming down with something," coryza, so we can have some runny nose. 02:22 Basically, they may think they either have the flu or because of the sore throat, they may think they have a strep throat. 02:29 Patients who are about to activate shingles, sometimes will simply only feel tingling right prior to the eruption of the legions in that dermatome distribution. 02:40 However, they may also have a short-lived viral syndrome. 02:44 Again, fever, cough, sore throat, rhinorrhea, and sometimes, they'll have cervical adenitis. 02:50 Location. 02:51 Chicken pox lesions, again, coming after a complete total systemic viremia will be anywhere and everywhere. 02:59 Most often, they start up at the head. 03:02 In fact, the pearl for those of you who enter pediatrics, the place to look for a chicken pox lesion is behind the ear. 03:10 Many times, those lesions hide there, certainly up in the scalp area covered by hair. 03:15 And then you may see them very rapidly, over the course of a day, erupt sort of throughout the body, but from head down to toe. 03:22 Many times, they'll start centrally and then they'll move out peripherally to the arms, the legs, etc. 03:29 Shingles, again, is a dermatomal distribution, very often seen on the face, many times on the chest, sometimes toward the back. 03:39 It's rare to actually have a purely trigeminal nerve reactivation. 03:44 The progression for chicken pox. 03:46 One will see these lesions heal, but in different stages, and so, many times the patients seek care after the first eruption of lesions has occurred, and you have to distinguish a chicken pox case from some of the other blistering viral illnesses. 04:03 The key here is to find vesicles in different stages of healing. 04:08 So you may see an early macule, you may see a papule, you may see a vesicle with that clear, clouded fluid at the top. 04:15 You may see it already start to crust and look kind of like a bacterial pustule, or you may see a, sort of, hemorrhagic crusting lesion, which is to the final stages of recovery. 04:25 In shingles, the lesions are very painful. 04:28 They burn. 04:29 They're almost like a painful itching. 04:32 It's a deep, burning itch. 04:34 And the lesions themselves will be in a dermatomal distribution, once again, but look more hemorrhagic than they do with the chicken pox. 04:43 So, here we have description and pictures of the lesions. 04:46 So on the lower left side, the image shows typical varicella chicken pox lesions in differing stages. 04:54 The classic description, and you'll see this historically as well as today, of a chicken pox lesion at its primary stage is "dew drop on a rose petal." A drop of dew, clear fluid dew on a rose petal. 05:07 Faint erythematous. 05:09 It's beautiful, except that itches like you wouldn't believe. 05:12 On the right lower part of the slide, you see a shingles activation in a dermatomal distribution, right? You can see that specifically in just 1 part of the face. 05:22 It's on only 1 side of the face It's unilateral. 05:26 If you see lesions like that crossing the midline, meaning both sides of the body, that is not going to be shingles. 05:32 That'll be some other disease process.
About the Lecture
The lecture Varicella-Zoster Virus (VZV) – Herpesviruses by Sean Elliott, MD is from the course Viruses.
Included Quiz Questions
Which of the following best describes the vaccine used for the prevention of infection by varicella-zoster virus?
- Live-attenuated
- Inactivated whole-cell
- Toxoid
- Conjugate
- Fractional
Which of the following is the most likely diagnosis for a child presenting with vesicular lesions all over the body in different stages of healing?
- Chickenpox
- Roseola
- Measles
- Shingles
- Rubella
The classical distribution of the maculopapular rash due to reactivation of infection by varicella-zoster virus in an adult is justified by which of the following?
- Dermatomal pattern
- All over the body
- Face and trunk
- Palms and soles
- Scalp and back of the neck
Author of lecture Varicella-Zoster Virus (VZV) – Herpesviruses

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
