Playlist
Show Playlist
Hide Playlist
Ulnar and Radial Nerves – Nerve Lesion of Upper Limb

-
Slides 10 UpperLimbAnatomy Pickering.pdf
-
Download Lecture Overview
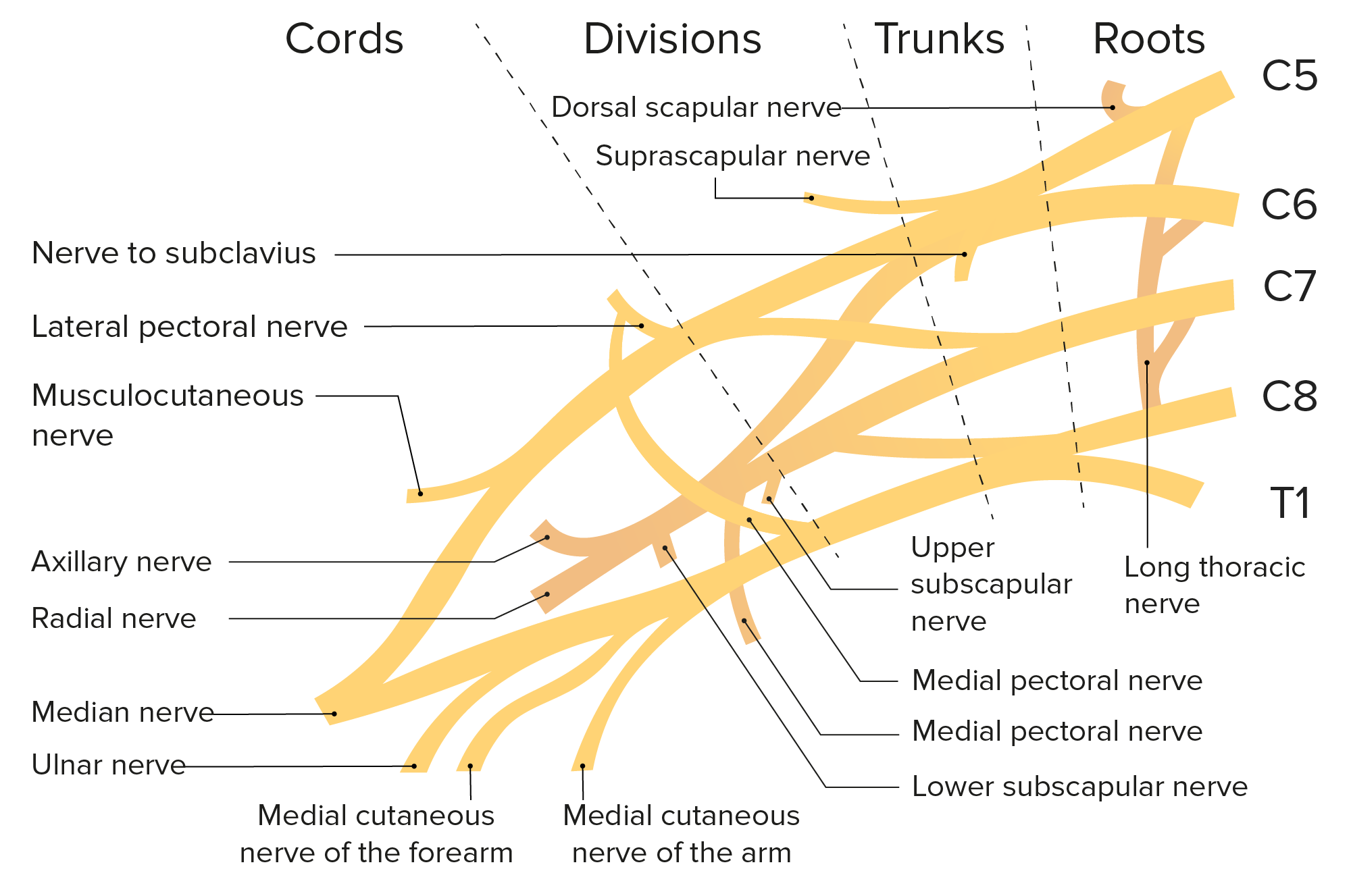
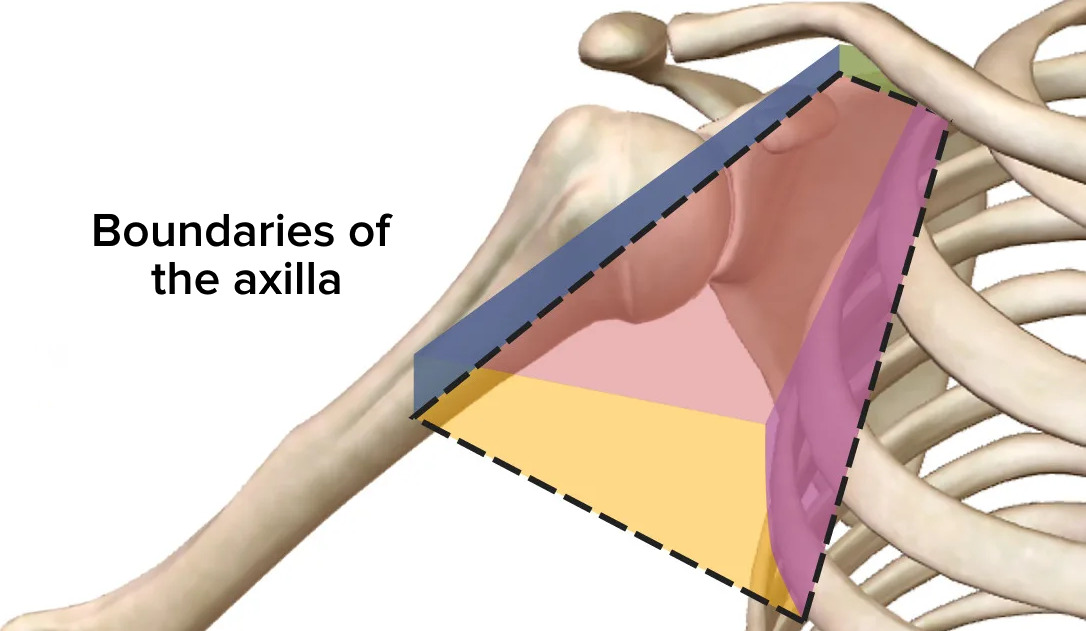
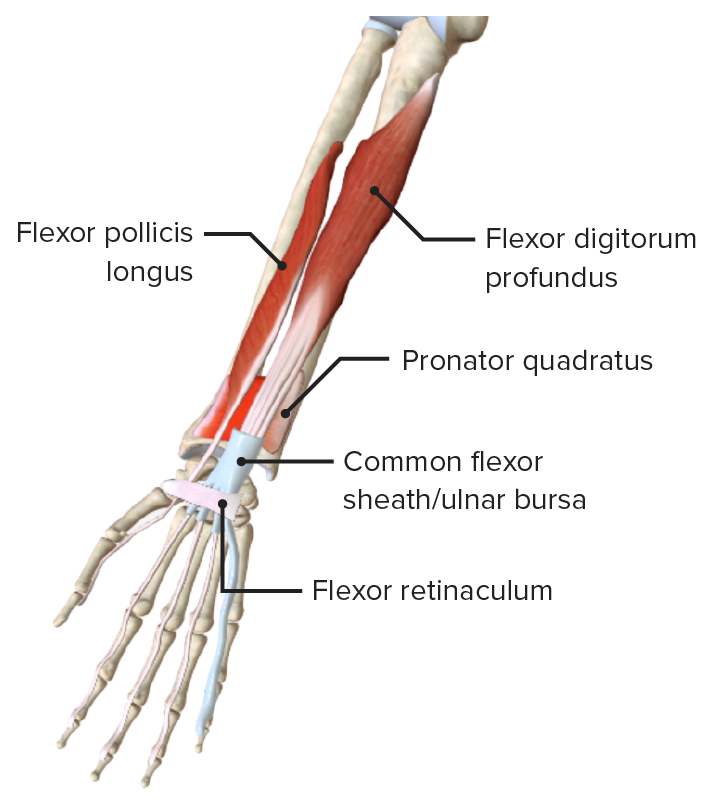
00:00 Now let’s move over to the ulnar nerve. The ulnar nerve passes close behind the medial epicondyle of the humerus, and then it runs again within the anterior compartment of the arm alongside the ulnar artery. It doesn’t pass through the carpal tunnel, but it runs superficial to the flexor retinaculum in Guyon's canal or the ulnar canal to go and supply some muscles within the hand. But damage to the ulnar nerve and this can be as it passes posterior to the medial epicondyle, are likely placed, or compression at the elbow or Guyon’s canal can lead to damage. Sensory loss, this will be at the medial surface of the palm, the medial one and a half fingers, those fingers that were preserved when we had median nerve damage. So the median nerve did three and a half. The ulnar nerve is redoing the remaining one and a half for finger 5 and the medial surface of 4. So you’ll lose sensation there. You’ll also have paralysis of the vast majority of those intrinsic hand muscles. So the medial to lumbricals, the interossei, the hypothenar eminence muscles, these will be paralyzed with the effects on functionality. The hand will be deviated to the radial side when a fist is formed because flexor carpi ulnaris is no longer able to make a even flexion of the wrist. So the radius via the flexor carpi radialis muscles will pull it towards the radial sides so it have radial deviation. 01:37 And you’ll have an inability to flex fingers 4 and 5, and also the distal interphalangeal joints. And these are what supplied by flexor digitorum profundus, the ulnar belly, the ulnar nerve supplying the bellies to these digits. So this time, when a patient forms a fist, digits 4 and 5 remain extended at the distal interphalangeal joint, yet the remaining fingers are flexed. Then you have what’s known as claw hand. 02:07 If we now move on to the radial nerve, the radial nerve passes to the posterior compartment of the arm where it supplies triceps, and then it supplies the posterior surface of the forearm, where we can see it here. It’s passing from the posterior cord. It passes the triceps muscle which it innervates. It then runs onto the posterior surface of the forearm supplying the extensor compartment. Damage to the radial nerve can be via a knife injury perhaps in the axilla or a humeral fracture where the shaft of the humerus is damaged. Paralysis, well, if the damage to the radial nerve occurs superior to the origin of the branches that supply triceps, then triceps brachii, brachioradialis, supinator, and the extensors of the wrist will all be damaged. 03:00 So if the lesion is high up, say it’s a humeral fracture before it has given off the branches to triceps, then every muscle distal that it supplies will be affected. 03:11 And this can have the effects of what’s known as wrist drop. We can see we’ve got an inability to extend the wrist because the extensor muscles in the forearm are damaged. You may also have an inability to extend the forearm at the elbow joint if triceps is damaged. 03:29 So you’ve got wrist drop primarily as the problem with a radial nerve lesion. This is due to paralysis of the extensors, and therefore, you have unopposed tonic contraction of the flexor muscles, and that leads to this flexed wrist drop position. Sensory loss is going to be over the lateral aspect of the dorsal of the hand, and you can just see a small little region here which is affected by the sensory loss due to damage to the radial nerve. So let’s have a look at the axillary nerve.
About the Lecture
The lecture Ulnar and Radial Nerves – Nerve Lesion of Upper Limb by James Pickering, PhD is from the course Upper Limb Anatomy [Archive].
Included Quiz Questions
Which statements regarding the ulnar nerve are true? Select all that apply.
- It passes posterior to the medial epicondyle.
- It passes beneath the flexor retinaculum.
- It runs medial to the ulnar artery.
- Injury causes sensory loss over the medial palm and medial one-and-a-half fingers.
- It derives from the median nerve.
Which muscles will be affected by injury to the radial nerve due to fracture of the humerus? Select all that apply.
- Triceps
- Biceps
- Brachioradialis
- Supinator
- Extensors of the wrist
Author of lecture Ulnar and Radial Nerves – Nerve Lesion of Upper Limb

James Pickering, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
