Playlist
Show Playlist
Hide Playlist
Other Causes of Dementia

-
Slides 02 Dementia Neuropathology II.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
00:01 Here, we’ll take a look at Pick’s disease. 00:03 Pick’s disease really is a name that’s falling out of favor. 00:08 The one that you definitely want to know, and the one that makes much more clinical sense is frontotemporal dementia, FTD. 00:17 Rare, compared to Alzheimer’s disease. 00:21 Rare, but yet know everything about F – Frontal lobe, T – Temporal. 00:28 So, you tell me, if you have problems with the frontal lobe, how are you going to behave? Like, Dr. Raj, crazy, insane, mood, behavior, instability. 00:37 Right? That’s frontal. 00:39 What about temporal? We’ll see that in a second. 00:41 Think about temporal. 00:42 Language center? There you go. Good. 00:45 Frontotemporal dementia. 00:47 And that’s what you’re going to predict. 00:48 Clinically, often have a combination of frontal and temporal. 00:52 Frontal lobe includes personality changes, mood behavior or disorders, poor judgment, disinhibition. 01:00 Does this sound like me? Temporal lobe, we have disturbances predominantly of the language. 01:06 Frontotemporal dementia, rare. 01:10 Frontotemporal Dementia or Frontotemporal lobar degeneration (FTLD) is broken down into three major subtypes based on the dominant proteins found in brain inclusions. 01:21 The first subtype, FTLD-tau, represents about half of FTD cases. It's characterized by hyperphosphorylated tau proteins that have become insoluble. Normally, tau proteins help stabilize the cell's structure, but when they're hyperphosphorylated, they lead to cellular dysfunction. 01:40 The second subtype, FTLD-TDP, accounts for roughly 40% of FTD cases. 01:46 This subtype involves TDP-43 proteins that are also hyperphosphorylated and insoluble. 01:54 In healthy cells, TDP-43 is involved in regulating how genetic information is used, but in FTD, the protein's abnormal form disrupts this process. 02:03 The third subtype is FTLD-FET, which includes 5 to 10% of FTD cases. 02:09 This subtype has inclusions of FET proteins, which are associated with RNA and DNA binding and are essential for normal cell function. 02:18 Let me quickly go through this with you. 02:20 So grossly, what are you going to find here? Well, I told you this is a differential of Alzheimer’s disease. 02:26 There is going to be -- as opposed to global atrophy that we saw with Alzheimer’s disease, with the frontotemporal dementia, you’re going to find asymmetrical atrophy. 02:36 What does that mean? It means that you’re not going to have the same type of global atrophy. 02:40 You might find deepening of the sulci in some places but not in others And often, it will spare the posterior two-thirds of the superior temporal gyrus, and that’s important. 02:50 So, there’re sparing here. 02:52 Severe atrophy results in gyri. 02:55 Well, what happens? The gyri is going to thin, and then you have a knife-like appearance that you’re going to find because it looks like you’re cutting right through, cutting right through. 03:05 Microscopically, severe neuronal loss as you can imagine, especially in the outer three layers of the cortex. 03:11 And you have these things called Pick cells, and this I would know. 03:16 These are neuronal swellings that you find with frontotemporal dementia. 03:20 Remember, rare when compared to Alzheimer’s disease. 03:23 So, if you’re suspecting frontotemporal dementia, make sure that you’re darn sure that this is what it is because they’re going to give you specific information. 03:31 They have to. 03:32 So, there’s no really such thing as your plaques, things of that nature, but you will find tau, so be careful there. 03:42 The Pick bodies, well, it's cytoplasmic, round to oval, filamentous inclusions, which are very weakly eosinophilic. 03:50 What color is eosinophilic? Pinkish. 03:53 But stain strongly with silver stain. 03:55 Now, be careful with that. 03:56 Last time we saw silver stain was actually of the beta-amyloid plaque. 04:01 Composed of neurofilaments, vesiculated type of endoplasmic reticulum, and paired helical filaments that are similar to those found in Alzheimer’s disease referring to the tau. 04:12 So be careful there, please. 04:13 You really, really want to pay attention to that asymmetrical type of atrophy that you find with frontotemporal dementia. 04:20 In Alzheimer’s, it’s more or less global. 04:24 This is a photomicrograph of the anterior cingulate cortex taken from a patient diagnosed with frontotemporal dementia. 04:30 The tissue specimen has undergone a specific immunohistochemical staining process, using an anti-tau protein immunostain, which appears brown, to label the abnormal tau proteins. 04:41 This has been counterstained with hematoxylin, which stains the cell nuclei and provides the blue background you see here. 04:48 As we look closer, you can observe many tau-immunoreactive dystrophic neurites. 04:54 These are characterized by the small, abnormally shaped brown-immunostained extensions emanating from the neurons. 05:01 In the inset, a magnified view, we identify a distinct tau-positive neuronal cytoplasmic inclusion. 05:09 This structure, known as a Pick body, is indicative of the disease and can be seen within what we refer to as a 'ballooned' neuron due to its enlarged size. 05:19 So, whenever you hear about tau, top on your differential should be, obviously, Alzheimer’s disease, rarely could be frontotemporal dementia. 05:31 Next, we move on to movement disorders. 05:33 In other words, these are subcortical dementia. 05:38 Let me stop there for one second. 05:39 What does cortical dementia mean to you? Cortical meaning higher, higher type of cognitive functioning, right? We talk about language and perception of language and being able to do those kinds of things. 05:52 Subcortical, you start getting closer to what can make your life easier. 05:56 Basal ganglia, Parkinson’s disease. 05:59 What do you know about Parkinson's? You lose the dopamine. 06:02 Multisystem atrophy. 06:04 Progressive supranuclear palsy, we’ll talk about. 06:07 Corticobasal type of degeneration, Huntington’s chorea, and Wilson’s disease are movement disorders that we’ll take a look at. 06:15 Our focus will be on basal ganglia, for the most part. 06:20 Let’s first begin our discussion by looking at Lewy body dementia. 06:25 Marked by progressive cognitive decline. 06:28 I’m going to show you something here that is a clinical pearl for sure, that you want to pay attention to with Lewy body dementia. 06:34 Memory and attention impaired. 06:37 Fluctuating course of good days. 06:42 This is what you’re paying attention to. 06:44 Your clinical pearl that you want to know for sure here with Lewy body dementia would be visual hallucinations. 06:51 Ha-Lewy-cinations. 06:54 Can you do that for me? Makes your life so much easier, doesn’t it? Ha-Lewy-cinations and delusions prominent and early feature, early feature. 07:03 That’s a big deal, and may present with parkinsonism. 07:09 So, what are we looking at in these pictures? Is it Lewy body? Specifically, they are in the middle. 07:14 Do you see that structure? That looks rather eosinophilic and pink. 07:17 Perfectly, perfectly circular. 07:19 That is something called a synuclein, synuclein. 07:23 I’ll talk to you about that in a second. 07:24 It’s important that you pay attention to synuclein. 07:27 Is it Lewy body dementia? And we have another structure that we’ll take a look at as well, and this is quite indicative. 07:34 Can you see that rod-like structure? That’s all for Lewy body dementia. 07:40 Cortical Lewy body must be present to diagnose definitively. 07:43 So, what is Lewy body? That’s what I’m showing you on the picture on your left. 07:47 Lewy body is composed of, that is what that circular eosinophilic structure that you’re referring to. 07:53 That is synuclein. 07:55 Memorize that. 07:56 Be able to identify it, please. 07:58 And overall, that circular eosinophilic structure that you’re finding in this bigger structure is the Lewy body. 08:07 Plaques and tangles are frequently present, identical to those seen in Alzheimer’s disease. 08:11 Please be really careful. 08:13 What you will not find, obviously, in Alzheimer’s disease will be Lewy body. 08:17 What are you paying attention too clinically? Ha-Lewy-cinations. 08:21 What is that that we are seeing circular? Synuclein. 08:24 What is the body? The Lewy body. 08:27 Is this Parkinson? Nope. 08:31 Vascular dementia, also known as multi-infarct dementia. 08:35 What does that mean? Number of blood vessels that are undergoing compromise. 08:39 And the number of blood vessels that undergo compromise will then cause decreased cognitive functioning. 08:44 Vascular, multi-infarct dementia. 08:47 Risk factors are those for any type of vascular disease. 08:50 Maybe seen with large artery stroke or severe subcortical disease, this is known as Binswanger’s. 08:57 Abrupt onset or more commonly, clinical pearl, step-wise progression is the key to diagnosis. 09:05 It’s slow. 09:07 But here, we have blood vessels that are being affected. 09:09 So maybe atherosclerosis resulting in stroke, hypertension. 09:13 If you go down into the subcortical region penetrating deep arteries, then you’re worried about things like Charcot-Bouchard aneurysm and lacunar infarcts. 09:24 Focal deficit on neurologic exam suggests the diagnosis. 09:28 Vascular dementia, a.k.a., multi-infarct dementia and step-wise progression are the key points on this particular slide. 09:38 We’ll move on to normal pressure hydrocephalus. 09:42 Okay. 09:42 Slow down here for one second. 09:44 There are couple of things that I want to make sure that we’re clear about. 09:47 Hydrocephalus has been a topic that we’ve covered in great detail. 09:49 We have talked about communicating hydrocephalus, which means what? Communicating. 09:54 You’re thinking about the flow or the path of cerebrospinal fluid. 09:59 You’re moving from lateral ventricle, third ventricle, fourth ventricle, bathing the spinal cord up through the subarachnoid and then going into the arachnoid granulation, right? Communicating, example would be post-meningitis, when you have scarring or fibrosis of the arachnoid granulation. 10:14 Maybe tuberculous meningitis. 10:16 If it's obstructive, or your non-communicating hydrocephalus, a list of differentials or large and wide, in which we have Arnold-Chiari or you have Dandy-Walker, you could have medulloblastoma. 10:28 We'll talk about a bunch of these causing obstructive. 10:30 But in those cases, what happens? You have increase in intracranial pressure. 10:34 Now, we talked about Alzheimer's disease in which we then have global atrophy of the cortex resulting in a compensatory ventricular enlargement or we call it compensatory ventriculomegaly. 10:47 Actually, I didn't even make that up. I kid you not. 10:50 It's called ventriculomegaly. How beautiful is that name? Yes, I'm a dork. But the point is that hydrocephalus ex vacuo. 10:57 In that case, we have intracranial pressure that is normal. 11:01 And here we have normal pressure hydrocephalus. 11:06 How is this possible? First, please be able to identify your patient. 11:10 Dementia, gait difficulty, and incontinence. 11:15 Please know the triad. No doubt, please now the triad. 11:18 Gait difficulty, incontinence, and this dementia is actually reversible. 11:24 So why is it normal pressure? Well, the concept is over a long period of time chronicity maybe there is adaptation that is taking place in the brain. 11:35 And with that type of adaptation, maybe the pressure now in the intracranium has actually become normal. 11:42 Lumbar puncture may reveal elevated opening pressure. 11:44 Now, you want to be really, really careful with this, right? Because if your pressure, intracranial pressure is elevated, you never do a lumbar puncture, you're going to kill your patient. 11:54 But here, if you know for a fact that there is no signs or symptoms of increased intracranial pressure, well just keep this in mind. 12:02 Prolonged CSF monitoring may reveal abnormal what's known as B waves. 12:08 Imaging will reveal enlarged ventricles, it looks like it's hydrocephalus, and your treatment is with shunting. 12:15 Okay, so even though you call this normal pressure hydrocephalus, there could be increased accumulation of fluid, so shunting is necessary. 12:23 And excellent success. And this is important, because you're able to then drain the fluid from your ventricles and such, you actually would be able to reverse the dementia, the gait difficulty. 12:37 That is quite rare. 12:38 So now, apart from the reversible type of dementia, as we've talked about, such as: B12 deficiency, hypothyroidism, Wernicke-Korsakoff, and so on and so forth. 12:46 There's every possibility that this could also be reversed, in normal pressure hydrocephalus with simple shunt placement.
About the Lecture
The lecture Other Causes of Dementia by Carlo Raj, MD is from the course Dementia. It contains the following chapters:
- Pick's Disease
- Subcordical and Vascular Dementia
- Normal Pressure Hydrocephalus
Included Quiz Questions
Which of the following pathological findings is important in the pathophysiology of Lewy body dementia?
- Synuclein
- Neurofibrillary tangles
- Amyloid precursor protein
- Beta-amyloid plaque
- Reed-Sternberg cell
A 65-year-old Caucasian man presents to his physician's office with memory problems. He has a history of poorly controlled hypertension, diabetes, and hyperlipidemia. His son, who accompanies him, states that the patient seems to be progressively worsening in a step-wise manner. What is the most likely cause of the patient's condition?
- Multi-infarct dementia
- Lewy body disease
- Frontotemporal dementia
- Pick disease
- Parkinson disease
A 55-year-old African American man is brought to your clinic. His daughter says that he has been acting strangely for the past several weeks. He has been forgetting activities of daily living and recently started using inappropriate language with his coworkers. What is the most likely diagnosis?
- Frontotemporal dementia
- Alzheimer disease
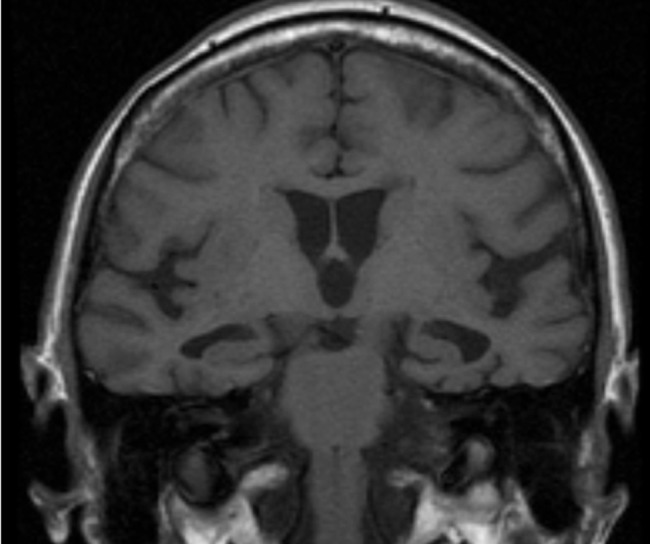
- Lewy body dementia
- Vascular dementia
- Multi-infarct dementia
Which of the following is NOT true regarding frontotemporal dementia?
- Atrophy of frontal and parietal lobes
- Atrophy of frontal and temporal lobes
- Neuronal loss in the outer three layers of the cortex
- Severe atrophy leads to knife-edge-like gyri.
- Strong silver staining of pick bodies
A 45-year-old man presents to your office with difficulty in maintaining his balance. He has been experiencing tremors in his fingers as well as gait problems. Upon further questioning, he says that he has been seeing strange things lately and is unable to remember his daily tasks. His medical history includes hypothyroidism and diabetes. What is the most likely diagnosis?
- Lewy body dementia
- Parkinson disease
- Pick disease
- Vascular dementia
- Frontotemporal dementia
Which of the following is NOT an example of a movement disorder?
- Multi-infarct dementia
- Multisystem atrophy
- Wilson disease
- Progressive supranuclear palsy
- Parkinson disease
Which of the following is NOT seen in normal pressure hydrocephalus?
- Shrinkage of ventricles
- Gait disturbance
- Incontinence
- Dementia
- "B waves" on prolonged CSF monitoring
Author of lecture Other Causes of Dementia

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Every lecture should be done like that ! Thank you very much doctor !
Great lecture just like all of his lectures. He is always very engaging.
He explains things really well, the repititon means I remember what he is saying, and his jokes do aswell. very clear and concise.
Dr. Raj lectures are always funny This lecture is short, provides key points, easy to remember Excellent explanation for the anatomical-clinical correlation
