Playlist
Show Playlist
Hide Playlist
Turner Syndrome: Signs, Symptoms and Diagnosis

-
Slides Turner Syndrome.pdf
-
Download Lecture Overview
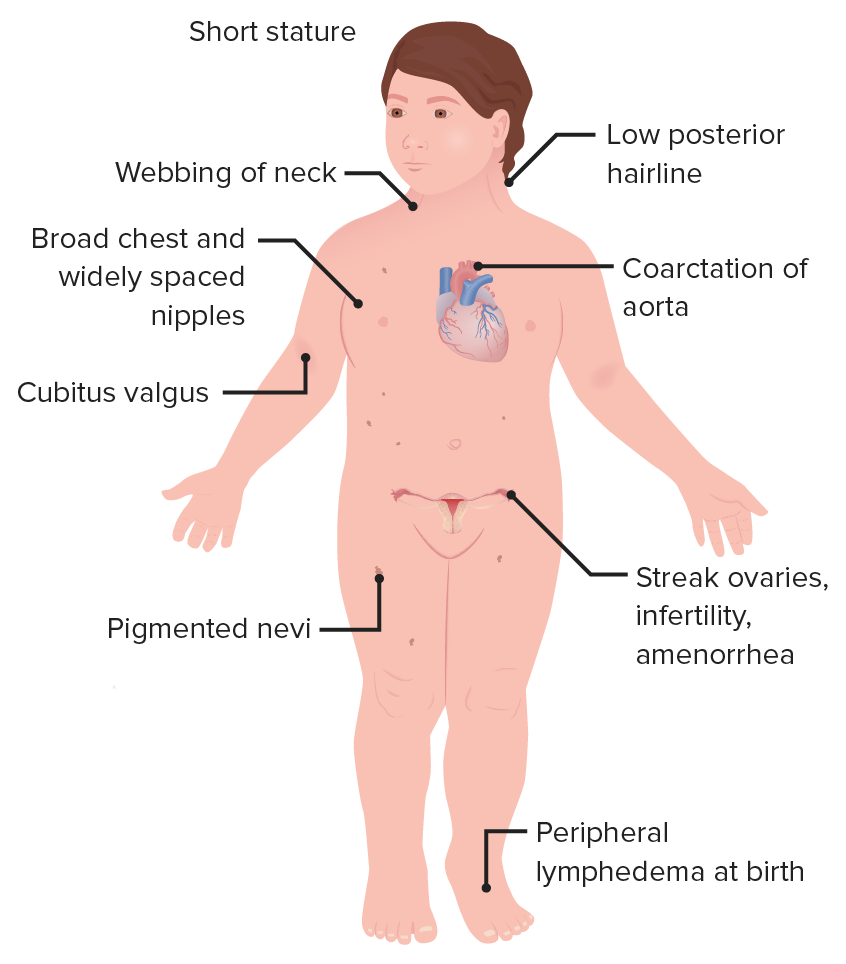
00:01 Hi. Let’s now review Turner Syndrome. 00:04 It’s really important that you pay attention to this lecture as you will find there are a lot of exam questions regarding this very rare syndrome. 00:12 How rare is it? Well, the incidence of Turner Syndrome occurs in 1 in 2,000 females worldwide. 00:20 Let’s now review the genetics of Turner Syndrome. 00:24 The X chromosome as you know, contains nearly 1,000 genes which relates to 5% of the total DNA in the cells. 00:32 That’s a lot. 00:34 So let’s review what we find normally. 00:37 In 46,XX individuals, one of the X chromosomes would be randomly inactivated. 00:44 With classic Turner Syndrome, the karyotype is 45,XO. 00:49 When I was a student, I remembered it as kisses and hugs. 00:52 45,XO from Tina Turner. 00:55 Maybe that will help you. 00:57 It’s one of the most common chromosomal abnormalities. 01:00 It occurs in 0.8% of all zygotes and is commonly found in spontaneous abortions. 01:10 Fewer than 3% of these zygotes will survive to term. 01:14 That means 37 weeks, making 45,XO, a common karyotype again found in spontaneous abortions. 01:24 Let’s review again a little bit more. 01:27 If this is too detailed for you, you can download the information and keep going. 01:32 The absence of the structure abnormality of one copy of the X chromosome is often due to nondisjunction. 01:40 This is a sporadic condition that’s possibly related to advanced paternal age. 01:45 But there are also reports that about 70% of the missing maternal X chromosome is why we have Turner Syndrome. 01:51 It’s actually not related to maternal age, but it’s possibly related to paternal age. 01:56 Let’s again review the cytogenetics of Turner Syndrome. 01:59 About half of patients with Turner Syndrome have a genotype of pure monosomy, which means they have a 45,XO karyotype. 02:07 Another half are mosaic, which means that some of their cells may be 45,XO and some of their cells maybe 46,XX. 02:14 The phenotype may be less pronounced in girls with 46,XX, 45,XO mosaicism. 02:20 But it varies depending on the timing and tissues affected by mosaicism. 02:25 And sometimes we find that patients have 46 X, Del (Xp) with the deletion of the short arm of the 2nd X chromosome. 02:33 The short arm is abbreviated p for petit. 02:39 With the Turner Mosaics, you can have 46,XY, 45,XO. 02:45 This is found in a minority of patients who have Turner Syndrome. 02:49 About 6-11%. 02:51 I doubt this would be on your exam but it’s important to know that these Turner Mosaics that have a Y chromosome, can actually be a ambiguous genetalia presentation. 03:04 If you’d like to know more about congenital adrenal hyperplasia and ambiguous genetalia, please download that lecture series. 03:11 Now, let’s go back to the cytogenetics of Turner Mosaics who have a Y chromosome. 03:16 They again can have a variable presentation with increased clitoromegally, which is a longer than normal clitoris or they can have ambiguous genetalia or they can have undescended testes or descended testes. 03:32 There is a critical need to assess for gonadoblastoma if a Y chromosome is present because 12% of these patients can have this tumor even at a very young age. 03:45 Lets now review the ABC’s of Turner Syndrome that is classically 45,XO or monosomy. 03:53 The ABC’s was actually created by a mentor of mine. 03:57 A stands for audiology. 03:59 These patients have hearing problems and can become deaf long term. 04:04 A stands also for autoimmunity. 04:07 So they have increased rates of rheumatoid arthritis, lupus, and other autoimmune diseases that can affect their overall health. 04:15 C stands for cardiac defects. 04:18 So these patients definitely need to be followed lifelong by a cardiologist. 04:23 D stands for dermatologic manifestations. 04:27 They can have pigmented nevi as you can see here, displayed in this cartoon. 04:32 They can also have failure to grow. 04:34 So they tend to have short stature. 04:37 The X chromosome has a series of genes called the SHOX genes and they are related to stature and bone and tendon formation which results in the deletion of the SHOX gene actually causes the short stature and failure to grow. 04:53 And lastly, they can have gastrointestinal diseases that need to also be managed. 04:59 Okay! With the Turner syndrome patients clearly they can have abnormal genetics, they can have metabolic disorders, they can orthopedic complications, they can have psychosocial manifestations of their disease as well as renal anomalies. 05:15 So pay attention, because this could be tested on your exam. 05:19 30 to 50% of those with Turner Syndrome will have a horseshoe kidney as the most common renal abnormality. 05:26 They can also have a reproductive and pubertal disorders and we do talk about this in another lecture called primary amenorrhea. 05:35 They can also have X-linked disorders. 05:38 Clearly this occurs because they only have one X chromosome. 05:42 When the normal phenotypic and genetic female has a 46,XX, so she has 2 X chromosomes making her less susceptible to X-linked disorders. 05:54 The presentation of Turner Syndrome upon delivery is sometimes vary depending on whether they are pure monosomy or mosaic. 06:04 But sometime you can see that 20% to 30% of the diagnoses are made in the neonatal period. 06:10 The mosaics tend to be diagnosed later in life. 06:13 Usually they fall off their growth chart and they’re discovered by their pediatrician. 06:18 35% again will present a short stature, likely because they've fallen off their growth charts. 06:25 That’s why the growth charts are important to follow. 06:29 30% will present as adolescents or young adult women who again have primary amenorrhea which means they’ve never had a period or they have a delayed puberty. 06:39 You can see here in this graphic, this young woman is short. 06:43 She has the stigmata. 06:44 She has the webbed neck, she has the broader chest, she has no breast development and you can see also the she has no pubic hair which you typically do see some pubic hair with the Turner Syndrome patient. 06:58 Now, again, let’s talk about some of the details that you see in a Turner Syndrome patient. 07:03 Prenatally, neonatally, and in adolescence. 07:07 This maybe a little too detailed for your test. 07:10 If you’d like to skip on ahead, you’re free to do so. 07:13 But let’s review now some of the details of a prenatal diagnosis of Turner Syndrome. 07:18 There are some ultrasound finding that we see and fetuses who present with Turner Syndrome. 07:24 Typically, during pregnancy you have a growth skin or anatomy skin. 07:30 These patients will be small and that is called intrauterine growth restriction or IUGR. 07:36 They will have a large septate cystic hygroma, which usually sits on the back of the neck. 07:41 During ultrasound you can see this. 07:43 And this is pathognomonic usually for Turner Syndrome. 07:47 They can just have some nuchal thickening which is seen upon ultrasound. 07:51 They can have a short femur, which actually correlates to short stature and they tend to have total body, lymphangiectasia and cardiac defects. 08:02 In the neonatal period, we can have some other physical findings. 08:06 So remember, in the prenatal period they have IUGR or growth restriction. 08:11 This leads to low birth weight. 08:13 They can also have some lymphedema of the lower and upper extremities. 08:17 This occurs in 30%. 08:20 They can have a webbed neck but sometimes that’s hard to see. 08:23 They can have a high arched palate so you need to open the mouth and examine the palate upon delivery. 08:30 They can have low set but prominent ears and they may have a low posterior hairline and micrognathia. 08:38 In adolescence, the most common presentation is short stature, followed by amenorrhea. 08:46 They can also lack secondary sexual characteristics and in this case that would be breast development. 08:52 30% of Turner patient undergo some type of spontaneous puberty, but may rest. 08:58 They may have not achieved a Tanner 5 stage breast and not achieve Tanner stage 5 escutcheon. 09:06 Let’s discuss in another lecture where we review thelarche and pubarche. 09:11 Let’s now review diagnosis of the Turner Syndrome patient. 09:15 So if all the blood test come back normal and it's 46,XX, but she still have a strong clinical suspicion, you should do a tissue biopsy or tissue sample to actually look for the karyotype. 09:28 We should also always look for the Y chromosome with the use of FISH or PCR for the patient who has genitalia ambiguity. 09:38 There is no clinical warranty for routine testing for SRY or Y chromosomes and those who have 45,XO pure monosomy, without masculinization. 09:52 Let’s review short stature in Turner Syndrome. 09:54 So again, this is our patient who is short-statured and has all of the appropriate stigmata for Turner Syndrome. 10:01 She is short, she has the webbed neck, she has the broader chest, no sexual secondary characteristics that we can see. 10:08 They are shorter on average, 20 cm shorter, than their peers. 10:13 This cause a lot of distress in the patients and remember to be sensitive to that as you see these patients. 10:19 Remember, that they usually are born after having a diagnosis of IUGR or growth restriction that’s intrauterine. 10:26 They usually have a slowed childhood growth. 10:29 So as their peers are having their acceleration of growth which is the first sign of puberty, these girls are not growing. 10:36 They may have mild skeletal dysplasia, upper to lower ratios, and so, they again appear shorter. 10:45 Again, remember, and this is a high yield fact which could be on your exam, they lack the pubertal growth spurt that you typically would see during the puberty.
About the Lecture
The lecture Turner Syndrome: Signs, Symptoms and Diagnosis by Lynae Brayboy, MD is from the course Normal Puberty and Disorders of Sexual Development. It contains the following chapters:
- Genetics of Turner Syndrome and Turner Mosaics
- The ABC's of Turner Syndrome
- Turner Syndrome: Diagnosis
Included Quiz Questions
Which of the following karyotypes is associated with classic Turner syndrome?
- 45, XO
- 47, XXY
- Trisomy 21
- Trisomy 18
- Trisomy 13
Which of the following tumor is associated with Turner syndrome?
- Gonadoblastoma
- Pancreatoblastoma
- Hepatoblastoma
- Neuroblastoma
- Wilms tumor
Which of the following kidney anomalies is associated with Turner syndrome?
- Horseshoe kidney
- Autosomal recessive polycystic kidney disease
- Multicystic renal dysplasia
- Double ureter
- Congenital hydronephrosis
Which of the following symptoms and signs are NOT associated with Turner syndrome?
- The length of the arm span is greater than the patient's height.
- Webbed neck
- Broad chest and widely spaced nipples
- Cubitus valgus
- Low posterior hairline
Which vascular or heart anomaly is associated with Turner syndrome?
- Coarctation of aorta
- Patent ductus arteriosus
- Transposition of great vessels
- Ventral septal defect
- Atrial septal defect
Which of the following is NOT an ultrasound finding seen in fetuses with Turner syndrome?
- Snowstorm appearance
- Large septate cystic hygromas
- Nuchal thickening
- Short femur
- Intrauterine growth restriction
Which of the following is NOT typically found in neonates with Turner syndrome?
- Simian crease
- Lymphedema
- Webbed neck
- High arched palate
- Low-set prominent ears
Which of the following is the next best step for diagnosing a patient with all blood tests being normal but high clinical suspicion for Turner syndrome?
- Karyotype the cells
- Repeat all tests
- Check hormonal levels
- HLA typing
- DNA sequencing
Author of lecture Turner Syndrome: Signs, Symptoms and Diagnosis

Lynae Brayboy, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
