Playlist
Show Playlist
Hide Playlist
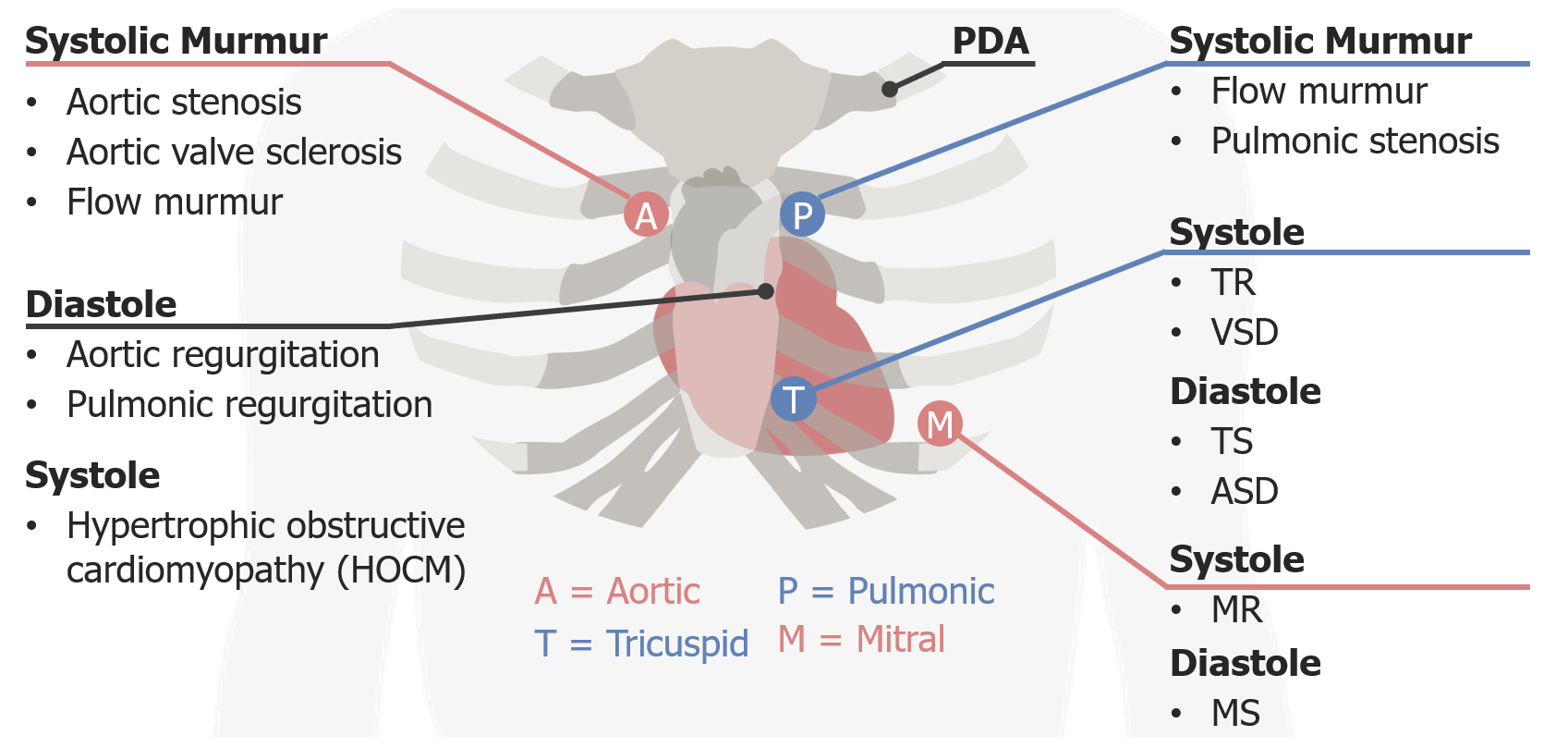
Tricuspid Regurgitation – Systolic Murmurs


-
Reference List Physical Examination.pdf
-
Download Lecture Overview
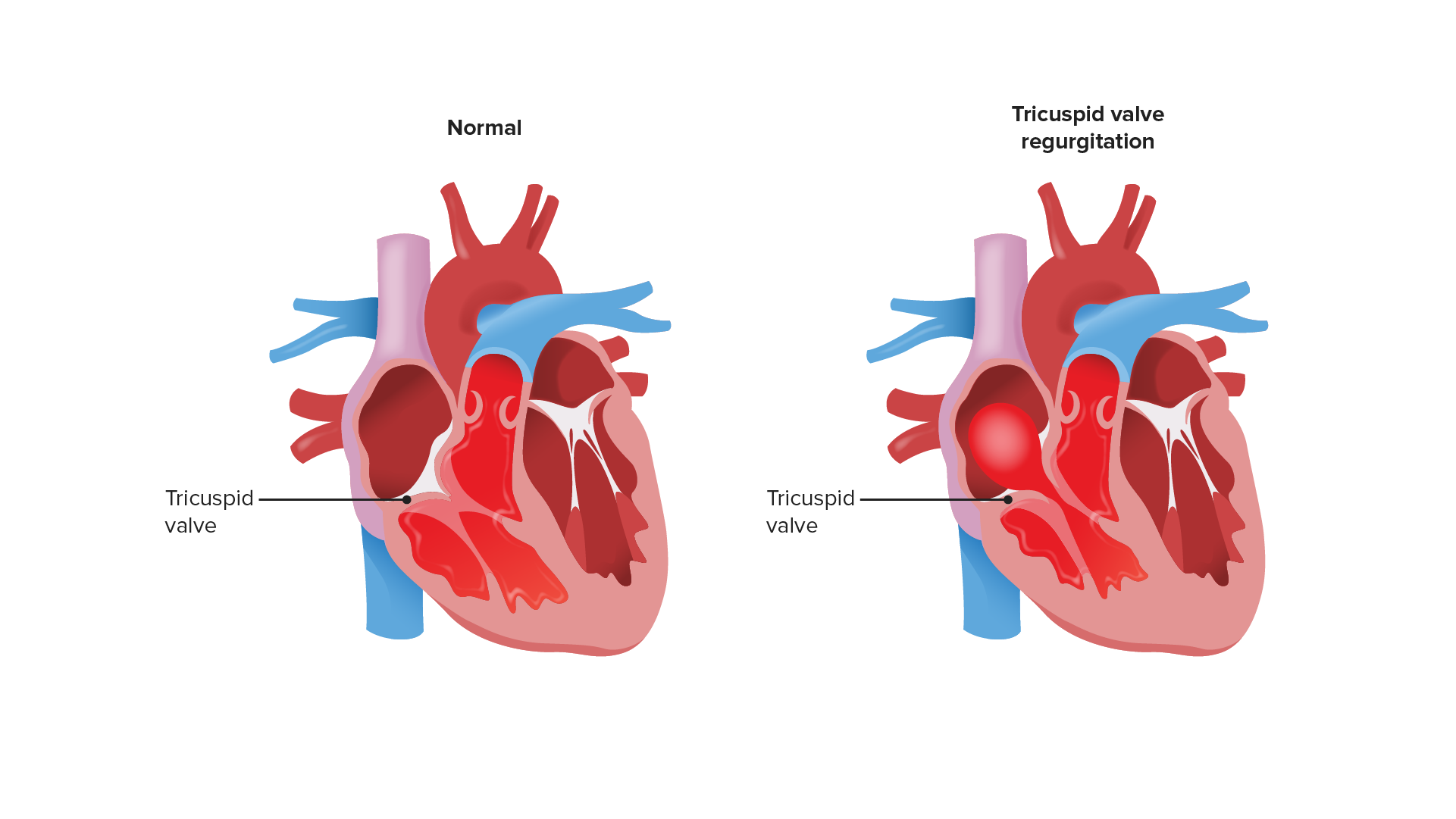
00:01 The next murmur that we should talk about is tricuspid regurgitation on the other side of the precordium. 00:08 The tricuspid regurgitation murmur has a lot of similar features with mitral regurgitation, it's high in pitch, it has a [making a sound] kind of wave form and the grade or intensity of the murmur that we hear does correlate fairly well with the extent of regurgitation in the tricuspid valve. 00:30 The location of course, is in the tricuspid area, which helps us out as well. 00:34 The real different feature of tricuspid regurgitation is that since it is a right-sided murmur, anything that affects preload, that is the blood returning to the right-side of the heart, could affect the volume or loudness of that murmur. 00:49 So in this instance, what we're going to do is very simple observation where when he just breathes, during inhalation, as we talk about before, when you inspire, you're creating a negative intrathoracic pressure, you're actually creating a small vacuum in your chest. 01:08 That vacuum is drawing blood, it actually sucks blood from your superior vena cava, and your inferior vena cava draws more blood to the right-side of your heart to your atrium, and then to your ventricle so if there's more blood in your right ventricle, when it squeezes, more of it is going to go forward but also more of it is going to go backward. 01:26 So simply this technique of paying attention to the respiratory cycle as he quietly inspires, quiet inspiration, will hopefully find that during the respiratory cycle there's variability in the murmur. 01:39 So with while listening to his tricuspid valve, I find that when he's just casually breathing at rest, the murmur gets louder during inhalation and a bit quieter during exhalation. 01:57 That feature of increased intensity with quiet inspiration would support a tricuspid regurgitation murmur. 02:05 Now you can imagine that if you've got a patient who's got a fever and potentially has a history of injection drug use and you're concerned about endocarditis, simply having a typical hollow systolic murmur at the over the tricuspid region especially if it exacerbates or is increased in volume with quiet inspiration that is a very high likelihood ratio in support of there being real tricuspid regurgitation and we'd, of course, be concerned about spontaneous bacterial endocarditis in a patient with a history of IV drug use.
About the Lecture
The lecture Tricuspid Regurgitation – Systolic Murmurs by Stephen Holt, MD, MS is from the course Examination of Cardiovascular and Respiratory System.
Included Quiz Questions
Which features are the MOST accurate descriptions of a tricuspid regurgitation murmur?
- Located at the tricuspid area, holosystolic, high-pitched
- Located at the apex of the heart, crescendo/decrescendo, the intensity of the murmur predicts the extent of valvular disease
- Located at the left lower sternal border, heard during diastole, the intensity of murmur does not correlate with the degree of stenosis
- Located anywhere in the chest, heard during systole, the intensity of murmur correlates with the degree of valvular disease
- Located at the right upper sternal border, diastolic, high pitched
Author of lecture Tricuspid Regurgitation – Systolic Murmurs

Stephen Holt, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
