Playlist
Show Playlist
Hide Playlist
Thyroid Storm & Subclinical Hyperthyroidism – Hyperthyroidism (Thyrotoxicosis)

-
Slides Hyperthyroidism incl. Graves Disease.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
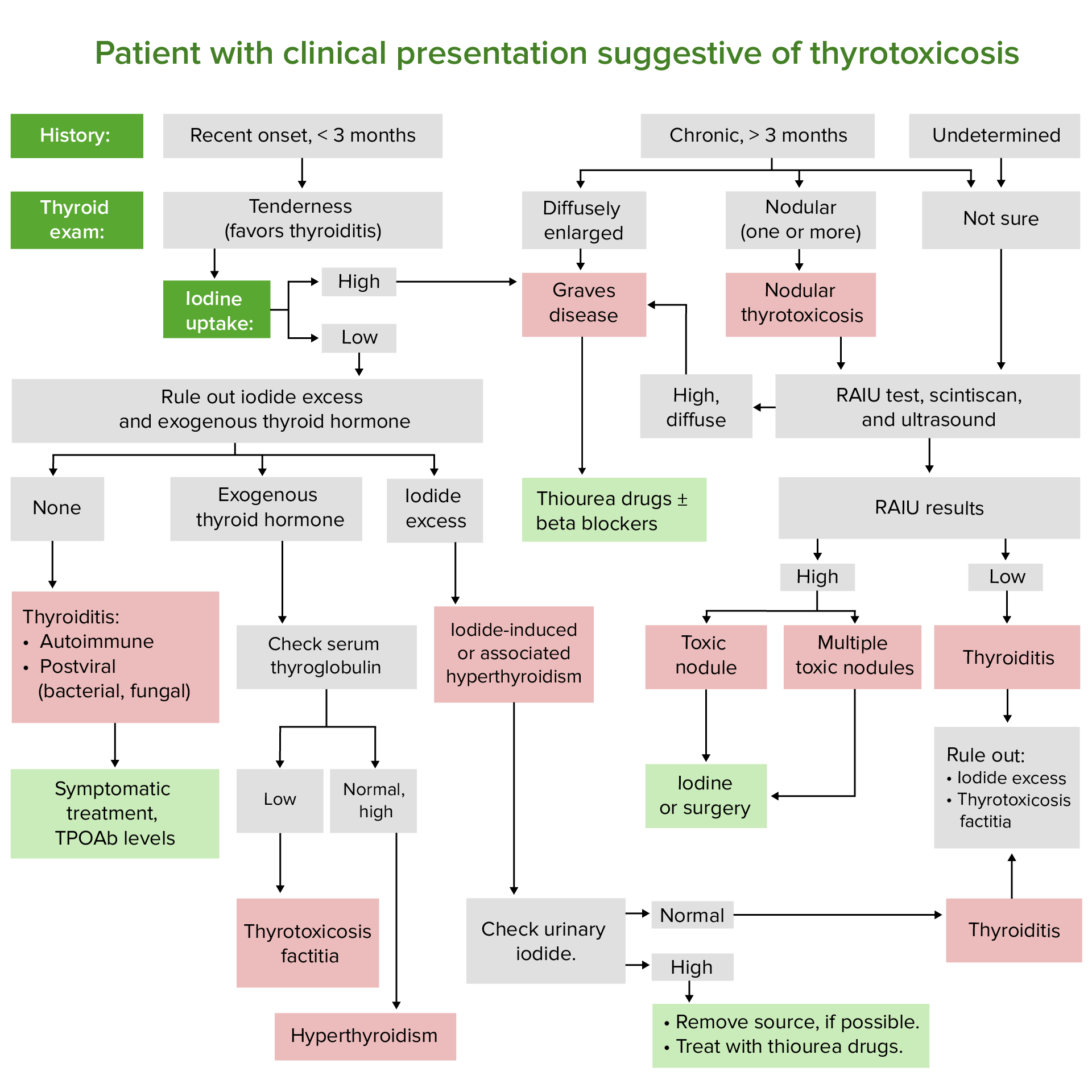
00:01 Thyroid storm, what happens here? Let’s say that the colloid gets destroyed. 00:06 When it does, it may then result in massive release of T3, T4 into circulation. 00:14 Characterized by fever, sever tachy-. 00:16 All that thyroid hormone sensitizing the heart and therefore, making it easier for catecholamines to work on beta-1 receptors to the point where the palpitations and arterial fibrillation might be taking place. 00:28 There might be so much issue then which now you might then cause delirium or to the point of even coma. 00:34 Quite dangerous – thyroid storm. 00:37 Usually, precipitated by severe physiologic stress (childbirth, surgery), lots of stress in a patient with uncontrolled hyperthyroidism. 00:49 Look for stresses in which the… results in massive release of T3, T4 into circulation. 00:56 With the thyroid storm, you want to try to get in there as quickly as possible, because you’re worried about the patient becoming unconscious. 01:04 Antithyroid drugs are the main therapy – should be started at least several hours prior to any, any iodine. 01:11 PTU is preferred mainly due to, once again, its inhibition of conversion of T4 into T3. 01:18 You’re worried about the palpitations, tachycardia and arterial fibrillation and therefore you’re thinking about giving beta blockade and “stress dose” of glucocorticoid coverage, because, remember, what is the precipitating event that is leading up to a thyroid storm? Extreme stress, such as childbirth. 01:38 And therefore, during this stress, maybe it will be in the best interest of the patient to therefore supplement the patient with more glucocorticoid. 01:51 Thyroid storm Potassium iodide can be used in the treatment. It is taken up by the thyroid and blocks the synthesis and release of additional thyroid hormone. 02:01 Administer 1 hour after PTU or methimazole because it may stimulate release of thyroid hormone at first Supportive measures, fluid and electrolyte management, address underlying stress (such as infection, maybe the childbirth we were talking about earlier) and make sure that you monitor the underlying issue before you completely relieve the patient of any therapeutic management. 02:24 Acetaminophen for that fever, not aspirin, because what does aspirin do with your thyroid hormone? Remember. 02:32 It may displace… Aspirin, NSAIDs may displace your thyroid hormone T4 from your TBG. 02:39 We’ve talked about that particular issue being called euthyroid hypothyroxinemia. 02:49 Cooling blankets, because there’s fever here quite high. 02:53 Sedatives for agitation. 02:55 Thyroid storm. 02:56 Let’s talk about subclinical hyperthyroidism. 02:59 What does it define as biochemically? Constellation of, well, there’s suppressed TSH with normal free T4 and T3 levels that are present. 03:10 Exogenous type – look at the number of patients that you might be exposed to in the US suffering from subclinical hyperthyroidism. 03:18 10 million in US, 200 million worldwide who take thyroid hormone are at risk. 03:27 So, those individuals… Hypothyroidism – extremely common. 03:31 Taking your levothyroxine and such may result in subclinical hyperthyroidism. 03:35 The benefit of inducing subclinical hyperthyroidism to suppress TSH in patients with thyroid cancer, nodular thyroid, head and neck irradiation outweigh the risk of administering thyroid hormone therapy. 03:49 So, often times, the benefit of inducing subclinical hyperthyroidism is to make sure that you suppress some of that TSH, as you expect to find here biochemically, especially in those patients that have thyroid cancer, nodules. 04:03 We’ve talked about multi nodular and head and neck irradiation outweigh the risks of administering thyroid hormone therapy itself. 04:13 The endogenous type – most common cause (mcc) would mean autonomously functioning thyroid adenoma or multinodular goiter. 04:25 Contribute to osteopenia, atrial fibrillation risk in the elderly. 04:30 Treatment is recommended in most patients with TSH<0.1, selected patients and especially those at high risk for osteoporosis and cardiac disease. 04:42 Subclinical hyperthyroidism is an area that you want to pay attention to, only because of its frequency found in our society. 04:51 Work-up of hyperthyroidism, step by step. 04:54 Presenting symptoms. 04:55 What would the presenting symptoms be in hyperthyroidism? Tachycardia, palpitations perhaps, tremors, anxiety, decreased weight. 05:04 If it’s a primary hyperthyroidism, you’d expect there to be suppression of your TSH with elevated levels of free T4. 05:14 Next, radioactive uptake and scan. 05:17 What you’re going to find? Let’s do the following. 05:21 If your thyroid gland is being destroyed, and we’ve talked about thyroiditis, and it would be in your best interest to make sure you go back in your organising your thoughts with thyroiditis. 05:33 Is it Graves’ disease? Is thyroiditis dealing with pain or is it painless? And if it is painful thyroiditis, is it acute, perhaps due to bacteria commonly? Or is it sub-acute, maybe due to mumps and coxsackie, viral? Or is it painless? In any case, whenever there’s thyroiditis, that means the thyroid gland has been destroyed. 05:58 And remember that graph that I showed you with a spectrum of symptoms that your patient may present and this may include what? Hyperthyroidism initially and then you get into euthyroid state transiently; may then get into hypothyroid and if it’s an infection may then result in recovery. 06:15 Point is this, if the thyroid gland is not functioning, how in the world is that thyroid gland going to take up radioactive iodine or any iodine at all? It’s not. 06:25 Decreased uptake in thyroiditis, but your patient’s presenting how? With hypothyroidism, sub-acute or silent with transient thyrotoxicosis. 06:36 Other possibilities. 06:38 All important. 06:39 Iodine-induced, meaning to say that iodine has been administered. 06:44 You increase production of T3, T4. 06:49 TSH is going to drop. 06:51 The TSH receptor is not being fully stimulated. 06:54 The radioactive iodine is therefore diminished. 06:59 Struma ovarii. 07:02 Why struma ovarii? The ovary in a female has an ovarian tumor known as cystic teratoma. 07:11 This teratoma is then going to directly release T3, T4. 07:16 Your patient is then going to present how? Hyperthyroidism. 07:21 It will supress TSH. 07:22 TSH receptor is sub-optimal functioning. 07:27 Decreased radioactive iodine uptake. 07:29 Exogenous, iatrogenic, factitious – all of it means synonymously that the patient is now taking T4. 07:40 How? Whatever means. 07:42 Maybe the doctor has prescribed levothyroxine. 07:45 Maybe an athlete might be taking some derivative of T3, T4. 07:50 Same concept. 07:52 Suppressed TSH. 07:53 TSH receptor not working. 07:54 What about radioactive iodine uptake? Decreased. 07:57 Do you see the similarities between iodine-induced, struma ovarii, exogenous administration? All resulting in decreased TSH receptor activity. 08:10 Let’s go on to the other side where now we have normal or elevated uptake of radioactive iodine. 08:17 Now, remember, this is not for therapy. 08:19 This is for what? This is for diagnostic purposes. 08:23 If you only find focal regions within your thyroid gland taking up your iodine, this to you means a “hot” nodule. 08:34 A “hot” nodule is benign, as far as you’re concerned. 08:39 It is not a cancer. 08:41 It’s that black and white for you right now. 08:45 Whereas if you had a nodule that is not taking up any iodine at all, how would that appear on an imaging study? An imaging study known as a scintigram, which show you a lucent area of being black. 08:57 That is a “cold” nodule and that to you should mean maybe your patient is suffering from cancer and the most common of all of your thyroid cancer would be a papillary cancer of your thyroid. 09:13 Localised focal regions of uptake. 09:17 Our next topic is what if the entire darn thyroid gland was taking up the iodine? The entire thyroid gland. 09:23 That means that every single TSH receptor is being stimulated, stimulated, stimulated, stimulated. 09:28 That means the entire thyroid gland pathologically is successfully taking iodine. 09:33 What kind? Radioactive. 09:35 So, therefore, what do you call this? A diffuse uptake. 09:38 Is that clear? Versus a focal uptake, “hot”. 09:43 Other possibilities, apart from Graves’ disease, would include: you can have choriocarcinoma and then with the choriocarcinoma you can either have the placental or the gestational cancer that you know of, or you’re going to have non-gestational choriocarcinoma and that choriocarcinoma would be a germ-cell tumor of either the testes or the ovaries. 10:06 With choriocarcinoma, when the time is right, you should know you divide that in gestational and non-gestational. 10:13 My point is this, in either case, chorio- means placenta. 10:17 You’re going to be releasing beta hCG in excess. 10:21 All that beta hCG shares a similarity structurally with what, what hormone? Good. 10:28 TSH. 10:29 Therefore, that beta hCG that’s being produced excessively in choriocarcinoma will then bind to TSH receptors, therefore cause what kind of uptake? A diffuse uptake. 10:40 Rare, but my goodness, isn’t that a good question? And then you have a secondary hyperthyroidism. 10:47 You have a pituitary tumor that is now a functioning adenoma producing too much TSH. 10:54 Secondary hyperthyroidism. 10:55 Now, you tell me: increased TSH receptor activity, increased radioactive iodine uptake – is it focal region or is it diffuse? Really, the TSH, it’s coming out of the anterior pituitary. 11:08 It’s not going to discriminate. 11:09 It will bind to as many TSH receptors as it needs to, on the thyroid gland. 11:13 Welcome to diffuse uptake. 11:16 How important is this algorithm for hyperthyroidism? Obviously, you want to spend time here and make sure that you have a full and complete understanding before walking into your board exam or walking into the wards of your hospital. 11:30 If this is in your head, can you see your patient literally falling into one of these boxes? That’s the way that you want to approach all medicine.
About the Lecture
The lecture Thyroid Storm & Subclinical Hyperthyroidism – Hyperthyroidism (Thyrotoxicosis) by Carlo Raj, MD is from the course Thyroid Gland Disorders.
Included Quiz Questions
A post-op patient presents with fever, tachycardia, and altered mental status. What thyroid condition must be on your differential?
- Thyroid storm
- Infectious thyroiditis
- Silent thyroiditis
- Plummer disease
- Graves' disease
What is included as part of the treatment of thyroid storm?
- PTU
- RAI
- Amiodarone
- Aspirin
- FNA
A patient is found to have suppressed TSH and increased T4 levels. What is the next best step in diagnosis?
- Radioiodine uptake scan
- Fine needle aspiration
- Blood cultures
- Glucocorticoid treatment
- Ultrasound
Which condition is not likely in a patient with decreased uptake on radioactive iodine uptake scan?
- Graves' disease
- Struma ovarii
- Silent thyroiditis
- Subacute thyroiditis
- Iatrogenic thyroiditis
Author of lecture Thyroid Storm & Subclinical Hyperthyroidism – Hyperthyroidism (Thyrotoxicosis)

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
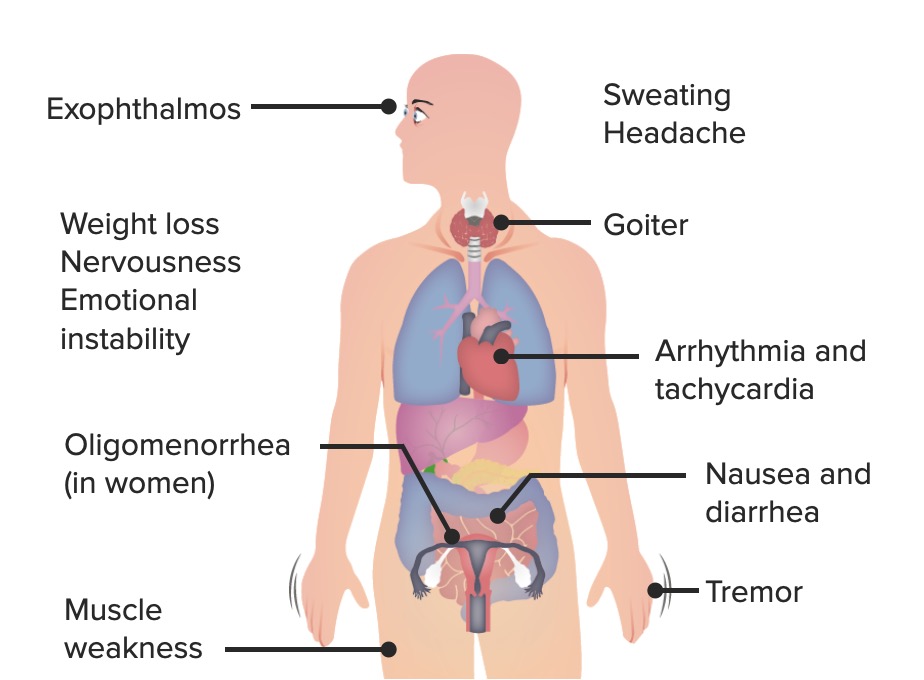
| 1 Star |
|
0 |
well explained and the difficult concepts were clearly explained such that is easier to remember. Dr Raj's energy when teaching is also remarkable!
