Playlist
Show Playlist
Hide Playlist
Thorax and Abdominal Wall Anatomy

00:01 We come now to the five primary muscles of the thorax. 00:04 They're innervated by the intercostal nerves, because they have attachment points to the ribs. 00:11 Here we see the external intercostal muscles running in this direction. 00:15 Because of this orientation, the lower portion is more flexible and therefore can pull the ribs upward. 00:21 This motion results in inspiration. 00:23 So the external muscles induce inspiration. 00:26 Deep to the externals, we see the course of the internal intercostals. 00:30 And right here, you can see the innermost intercostal group splitting off and coursing inwards. 00:36 Between indeed to the internal and innermost muscles, the costal groove is seen along the inferior rib border. 00:43 In this groove runs the neurovascular bundle. 00:45 From superior to inferior, you will find the vein, artery, and nerve. 00:50 So remember, VAN. 00:52 As they contract, the internal and innermost muscles pull the upper ribs inferiorly. 00:58 Therefore, inducing exploration. 01:00 The exception is a small portion of the innermost group which is cutaway here that lie between the hyaline costal cartilages. 01:07 They assist with inspiration because they pull the ribs upwards. 01:10 So the externals and the cartilaginous portions of the innermost group can provide inspiration. 01:17 These cartilaginous parts of the innermost muscles are sometimes called intercartilaginous muscles because they lie between the hyaline cartilages. 01:25 If we look now at the thorax from inside, we can see the course of the innermost intercostal muscles on the inside again. 01:34 Here you can see them splitting off the internal intercostals. 01:38 Running between the internal and innermost muscles on the lower edge of the rib in the costal groove, you can see the neurovascular bundle here. 01:46 Remember the order from top to bottom. 01:49 Vein, artery, nerve. 01:51 Here we see the intercostal nerve. 01:53 This nerve can cause intercostal neuralgia, a radiating pain that travels along the rib to the midline. 01:59 If the herpes virus is in the spinal ganglion, irritation to the skin, sun exposure or stress allows the virus to activate along the intercostal nerve distribution. 02:09 This results in a vesticular rash that's very painful and can become infected. 02:13 This is shingles, a disease caused by the Zoster virus. 02:18 So here again is the costal group containing the neurovascular bundle, Vein, artery, nerve, between the internal and innermost intercostal muscles. 02:28 Here we see the course of the innermost muscles. 02:31 If you look here, now, back and down at the ribs, we can see the subcostal muscles. 02:37 These are elongated internal intercostals, which only appear on the inferior posterior rib areas here. 02:43 Because this is the anterior thorax, they cannot be seen and are of no great importance. 02:47 They are often too small to even identify and some specimens. 02:49 Now, we see the fifth muscle from this group, the transversus thoracis muscle. 02:53 They course right and left like the fingers of a hand and tense the entire thorax facilitating exploration. 03:01 So let's summarize again. 03:03 The external intercostal muscles provide inspiration as do the intercartilaginous muscles. 03:15 Conversely, exploration is facilitated by the internal intercostals and the innermost intercostals. 03:21 The neurovascular bundle lies between the internal and innermost muscles. 03:25 The vein, artery, and nerve are protected within the costal groove. 03:29 Therefore, you should always make an incision or puncture on the superior edge of the rib to avoid disturbing the neurovascular bundle. 03:37 Then, you can actually disregard the subcostal muscles running along the posterior lower ribs. 03:44 And finally, we have the transversus thoracis muscle again. 03:47 The transversus thoracis, subcostals, internal and innermost intercostals are all expiratory. 03:55 Only the external and inner cartilaginous muscles are inspiratory. 04:01 All five primary thoracic muscles are innervated by the intercostal nerves and stabilize the entire thorax. 04:08 So the functions include inspiration, expiration, and Valsalva. 04:13 The transversus thoracis muscle on the right and left course inferiorly until they meet the transversus abdominus, the lateral oblique abdominal muscles. 04:25 Here we see the internal thoracic artery which runs inside the thorax. 04:30 It used to be named the internal mammary artery because it courses under the mammary glands. 04:35 This artery is the first branch of the subclavian artery that travels inferiorly. 04:40 And here it is prepared on the side of the sternal margin. 04:45 If we look inside the thorax, we see that it's covered by endothoracic fascia. 04:52 This is the thick lamina propria, a connective tissue. 04:56 The outer parietal pleura around the ribs is called the costal pleura. 05:03 The arteries endothoracic fascia covering ends distally but it is then covered by the transversus thoracis muscle. 05:10 It then passes over the diaphragm near the trigonum sternocostale. 05:16 And forms a confluence with the inferior epigastric artery which travels behind the rectus abdominus muscle. 05:22 This muscle also gives rise to the lateral umbilical plica. 05:28 Here we can see the inferior epigastric artery again within the rectus sheath and posterior to the rectus abdominus muscle. 05:36 The artery continues inferiorly and becomes the superior epigastric artery because it's now at the epigastric angle. 05:42 EPI is equal to the gas which means equal to the stomach. 05:47 Below the umbilicus, it is then called the inferior epigastric artery. 05:51 And here travels down to eventually flow into the external iliac artery. 05:56 This internal thoracic artery can be used as a coronary bypass artery. 06:00 And this is why it's the so called Clinton artery because he had the bypass surgery done using this artery as a graft. 06:07 We come now to the four secondary chest muscles. 06:10 Here we see the pectoralis major muscle. 06:14 Under the pectoralis major muscle lies the pectoralis minor. 06:19 Then here we see the serratus anterior muscle with its projections. 06:26 It attaches to the subscapularis muscle eventually and the posterior medial scapula. 06:33 The fourth smaller muscle, the subclavius, cannot be seen here. 06:36 We look at it instead on the other side. 06:39 We see the subclavius muscle here under the clavicle. 06:42 So that's the subclavius muscle. 06:44 Let's discuss all the secondary chest muscles in detail. 06:48 The pectoralis major and minor muscles are innervated by the medial and lateral pectoral nerve. 06:53 These nerves arise from the supraclavicular nerve which is a brachial plexus nerve. 06:57 The pectoralis major has three heads each with its own origin. 07:00 First, the pars clavicularis from the clavicle, the pars sternocostalis from the ribs and sternum, and the pars abdominalis from the anterior lamina of the abdominal rectus muscle. 07:10 A small portion also attaches on the front leaf of the rectus sheath. 07:13 Its fibers run along this axis turning 180 degrees at the insertion. 07:18 It forms the anterior axillary fold and inserts on the crista and greater tuberosity of the humerus. 07:26 Its function can be remembered by thinking of knotting a belt, internal rotation of the shoulder, arm flexion, and adduction. 07:34 The same motions used when tying a belt knot. 07:43 Now, if we fix the arm in place, the origin becomes the more mobile portion and can pull on the ribs. 07:50 This allows it to act as a secondary breathing muscle. 07:54 Below it, we find the pectoralis minor muscle. 08:01 It is innervated primarily by the medial pectoral nerve, but a small portion is done by the lateral pectoral nerve as well. 08:07 It originates from the second or third to the fifth rib and inserts on the coracoid process of the scapula. 08:16 Its function is to tilt the scapula forward and in short remains fixated to the chest wall if the other muscles fail. 08:24 If these other muscles fail, this scenario results in the scapula being pulled forward or anterior at the superior border, and the inferior angle protruding outward. 08:34 This is the so called winged scapula phenomenon. 08:39 The serratus anterior muscle that we see here has its origin from the first to the ninth rib. 08:54 It courses ventually to the subscapularis muscle and inserts onto the medial scapular margin. 09:00 It has three heads, a pars superior, pars media, and pars inferior. 09:05 The pars superior is the smallest. 09:07 It originates from the first and second rib above the superior angle of the scapula. 09:12 The pars media is also called the pars divergence because it diverges along the medial scapular border. 09:18 The pars inferior is the largest part. 09:21 And it's called the pars convergence because it converges towards the inferior angle of the scapula. 09:29 When contraction occurs, we see that it pulls the medial scapular border against the trunk. 09:34 We need this for example when pushing against something with outstretched arms. 09:41 So it fixes the medial scapula tightly to the trunk. 09:47 The lower portion on contraction pulls the inferior scapular angle laterally. 09:54 We need this when we lift our arms above the horizontal elevation position. 09:58 The upper part is antagonistic to this and functions to return the scapula back to the position when the arm is lowered. 10:04 The lower part pulls forward again and the upper part pulls backward. 10:08 When we support our arms, the origin becomes the more mobile part. 10:12 Since the origin is from the first nine ribs, the ribs can be elevated allowing inspiration. 10:19 That is why it's very important. 10:20 Actually, the most important, auxiliary or secondary respiratory muscle. 10:29 Because it lies here on the thorax, it's innervated by the long thoracic nerve, which arises from the brachial plexus as well. 10:38 Our fourth muscle, the small subclavius that we see here, comes from the first rib and inserts on the underside of the clavicle. 10:48 It helps stabilize the sternoclavicular joint and keeps the lumen of the subclavian vein open. 10:55 This is important because this vein is close to the heart and exposed to negative pressure. 11:01 When using a subclavian catheter, remember that air enters the vein and can cause an air embolism. 11:06 A subclavian catheter is a commonly used location for central infusion access. 11:17 The subclavius muscle is innervated by the subclavian nerve which arises from the brachial plexus as well. 11:24 When the clavicle is elevated, for example, by raising the arm to 180 degrees, the clavicle can be elevated to 60 degrees. 11:32 This stretches this muscle. 11:35 When it contracts, the clavicle is then depressed. 11:38 So its function includes, sternoclavicular joint stabilization, clavicle depression, and keeping open the lumen of the subclavian vein. 11:49 Here we see the thorax, the right and left lungs and in the middle, the heart and the mediastinum. 11:57 The lungs are located in the [hilum] pulmonis and the heart sits in between the right and left cavum pulmonis in the mediastinum. 12:06 In the right lung, we have three lobes. 12:10 Here you can see the upper lobe, here, the middle lobe, and here, the lower lobe. 12:15 When we do this as a learning aid, this is how the middle lobe sits. 12:18 Above this point is the upper lobe, then the middle lobe, then the lower lobe. 12:22 The left lung has only an upper and lower lobe. 12:26 When we look at the position of the heart, here you can see the pericardium. 12:35 If the pericardium is cut open, we can now see the heart inside. 12:41 It shifted 45 degrees to the left, rotated 45 degrees and angled 45 degrees down so that 1/3 is to the right of the sternum and 2/3 are to the left of the sternum. 12:54 Here we can see the aortic arch going off to the right. 12:58 This is the brachiocephalic trunk which then branches into the brachial artery, the subclavian artery, and the right common carotid artery seen running towards the head. 13:08 Because of these branches, it is termed the brachiocephalic trunk. 13:20 The second branch from the aortic arch is the left common carotid artery. 13:25 And the third branch is the left subclavian artery. 13:29 Here's a red metal wire in the aorta. 13:35 In this portion is the ascending aorta It comes directly from the left ventricle. 13:39 Then the arch bends itself downward and becomes the descending aorta. 13:42 At this level, it's called the thoracic aorta and it travels down towards the diaphragm. 13:49 We see the superior vena cava next to it. 13:54 The superior vena cava is formed by the confluence of the left brachiocephalic vein, which is cut off here and the right brachiocephalic vein. 14:03 So the brachiocephalic vein, as the name suggests, also gives rise to the subclavian vein in the internal jugular vein which converge at the venus angle. 14:13 Again, it's called the brachiocephalic vein because the subclavian vein comes from the brachium and the jugular vein comes from the head. 14:21 This is the angle of the veins. 14:23 But the lymphatic duct also joins on the right side from the posterior aspect. 14:30 The left vein angle is the confluence of the left subclavian vein, and the left jugular vein, and the thoracic duct. 14:37 This thoracic duct allows lymph back into the circulatory system. 14:46 If we look here, the superior vena cava continues to descend where it eventually empties into the right atrium. 14:53 This is what we see here. 14:55 From the atrium it goes into the corresponding right ventricle to a leaflet valve on the right side of the heart called the tricuspid. 15:07 Some use the learning aid, D for right. 15:10 D like Dexter, D like three or tri. 15:12 So the tricuspid lies on the Dexter or right side of the heart. 15:17 We have chordae tendineae threads here which connects the valves to the papillary muscles seen here. 15:26 We have three papillary muscles because we also have three cusps on the tricuspid valve. 15:31 These three cusps are the leafs that formed the valve. 15:33 From here on the right ventricle, we see the blue wire as it goes up over the pulmonary trunk, which then branches into the pulmonary arteries. 15:43 These arteries run up behind the aortic arch and superior vena cava to the right. 15:51 And we see the other pulmonary artery here coursing to the left. 15:57 The pulmonary veins return the blood from the lungs, but we have not yet seen that structure. 16:02 The pulmonary veins then empty into the left atrium. 16:05 Blood then flows from the left atrium into the left ventricle. 16:09 And from the left ventricle it flows out of the heart via aorta. 16:14 So the superior vena cava brings the blood into the right atrium. 16:17 From the right atrium, it goes into the right ventricle. 16:19 From the right ventricle, it exits via the pulmonary trunk, Then, to the pulmonary arteries, and into the lungs. 16:25 It returned from the lungs via the pulmonary veins, empties into the left atrium, and from the left atrium, it goes into the left ventricle. 16:32 Here you can see where my tweezers are pointing. 16:34 and I can grasp the red thread. 16:36 This is where it enters into the left ventricle. 16:38 From the left ventricle it goes out here via the aorta. 16:42 Now, we come to the abdominal muscles. 16:44 There are three groups. 16:45 An anterior group, a side oblique group, and a rear group with a muscle that we can't see here. 16:54 Let's start with the anterior group. 16:55 This includes the rectus abdominus muscle. 17:00 That washboard abdominal muscle which can be trained to show the intermediate tendons. 17:06 There can be three or four distinct levels and it's not always symmetrical. 17:13 The rectus abdominus muscle is also located within a rectus sheath. 17:17 With a lamina anterior, and a lamina posterior. 17:25 So front and back leaf that envelop the rectus abdominal muscle. 17:29 This is formed in part from the right and left three lateral oblique muscles. 17:36 In addition to the rectus abdominus muscle, this anterior group also includes the pyramidalis muscle which we can't see here. 17:43 It lies in the rectus sheath in front of the rectus abdominus muscle. 17:46 It comes from the pubic symphysis and forms a kind of pyramid shape that spans the linea alba. 17:51 The linea alba is the middle interweaving line between the right and left lateral oblique muscles. 17:58 The origin of the rectus abdominus muscle is up here, along the costal cartilages of ribs five to seven along the cycloid process. 18:13 Then it runs distally as the right and left muscles taper ultimately terminating at the pubic symphysis It functions in ventral flexion when the pelvis is fixed. 18:28 Or pelvic elevation when the upper body is fixed. 18:34 In most cases, it will not be actively involved in the abdominal crunch. 18:38 But rather just passively bulge that this may not be true in highly trained athletes. 18:45 Behind the rectus abdominus muscle lies a very important artery that we see here. 18:49 This is the inferior epigastric artery. 18:53 It plays an important role in the inguinal canal. 18:56 Besides it, we have the fossa inguinalis lateralis and medial to it, the fossa inguinalis medialis. 19:02 See the inguinal canal? The inferior epigastric artery travels in the rectus sheath behind the rectus abdominus muscle. 19:09 It is called the superior epigastric artery went above the navel and is not visible here at the level of the diaphragm through the sternal costal triangle. 19:23 As it passes through the Larry Fisher, it then merges into the internal thoracic artery also known as the internal mammary artery which lies behind the ribs about two or three centimeters lateral to the sternal margin. 19:34 This artery is often used in bypass grafts such as coronary bypass of the heart. 19:41 Let's discuss the rectus sheath structure. 19:43 It's very simple. 19:45 That's the rectus abdominus muscle. 19:47 That's the middle of the oblique. 19:49 And that would be the internal oblique muscle. 19:51 It courses forward and backwards to the rectus sheath. 19:55 The externus comes in superficially and attaches to the anterior leaf. 19:59 The transversus abdominus lies completely inside the sheath and only attaches to the posterior leaf. 20:04 These relationships, internal to the front and back, external only to the front, and transverse only to the posterior applied to the region above the navel down to the so called arcuate line. 20:19 Below this level, all three lateral muscles pass into the anterior leaf of the rectus sheath. 20:26 We will see this clearly in the inguinal canal. 20:39 Now, we come to the three oblique or lateral abdominal muscles. 20:42 Here we have the external oblique muscle that follows a line similar to placing our hands in trouser pockets. 20:49 It runs from the ribs to the inguinal ligament in the anterior superior iliac spine. 20:55 Underneath, lies the abdominal oblique muscle. 20:59 It has fibers that run downwards, transversely, and some even slightly upwards. 21:05 Finally, deep to the abdominal oblique. 21:07 We see the transversus abdominus which only has transversely oriented fibers. 21:13 During an appendectomy, an alternating incision is made to transverse these muscles. 21:18 The externus is cut in one direction, then the internus and another, and then the transversus is cut back in the original incision orientation. 21:25 Beneath the transversus, there's a connective tissue called the transversalis fascia. 21:29 Under which, you'll find the peritoneum. 21:31 Now let's go into more detail. 21:33 The external abdominal oblique originates from the ribs. 21:38 Its fibers are transversely oriented from seven points, on the sixth rib to the 12th rib. 21:47 It alternates distally with the latissimus dorsi, and proximately, with the straightest anterior muscle. 21:52 This creates the linea serrata. 21:57 Above the externus with the serratus anterior, below externus with the latissimus dorsi. 22:05 The fibers then traveled down radiating towards the iliac crest, lateral to the intestinal crest, to the anterior superior iliac spine and into the inguinal ligament. 22:16 It has an aponeurosis or flat tendon that splits here into a medial and lateral crus. 22:23 These are usually not clearly visible and abridged by intercrural fibres, the superficial abdominal fascia. 22:29 This fascia creates the superficial inguinal ring which is more pronounced in men. 22:35 Here we have a female specimen so it's harder to see. 22:40 The function of the external abdominal oblique, because it lies in front of the flex x axis is ventral flexion. 22:48 It can also do lateral flexion because it's oriented sideways. 22:52 Finally, it can function together with the internus of the opposite side to rotate the trunk. 22:57 The internus turns the trunk to the same side. 22:59 While the externus is rotates the trunk to the opposite side. 23:02 This side here would be fixed and that would be mobile. 23:10 This is why the trunk is rotated to the opposite side. 23:15 In addition, of course, it does the stomach press. 23:19 Below the external abdominal oblique lies the internal abdominal oblique. 23:24 Its original is not on the ribs as with the externus but down here, along the anterior superior iliac spine on the lateral edge of the inguinal ligament, and from the intermediate line on the iliac crest. 23:37 It has fibers that travel down and which join the transversus below here, below the ASIS. 23:46 It has fibers that run transversely, and it has fibers that run upwards to the lower edges of the three ribs. 23:56 As before, its function is like externus, ventral flexion, lateral flexion and the lower part turns the trunk to the same side. 24:09 By working with the externus to the opposite side, you can do trunk rotation. 24:12 It also is involved with the belly press. 24:15 The transversus abdominus now lies on the internal abdominal oblique Its fibers originate from the lower six ribs and that lies on the inside of the iliac crest. 24:32 Here, it originates from the internal inguinal ligament, and joints here below the ASIS with the internal abdominal oblique. 24:39 Both of these muscles are also raised so that there's a weak point on the abdominal wall that an inguinal hernia can rupture through. 24:48 The transversus runs in the direction of the linea alba. 24:51 It's the main muscle of the abdominal press. 24:55 They are the important points of the three oblique lateral abdominal muscles.
About the Lecture
The lecture Thorax and Abdominal Wall Anatomy by Prof. Dr. med. Steffen-Boris Wirth (EN) is from the course Gross Anatomy: In the Lab.
Included Quiz Questions
Which statement best describes how the external intercostal muscles assist with inspiratory respiration?
- They have their origin more ventral and distal than their attachment on the next lower rib and thus lift the thorax during contraction.
- They have their origin more ventral and distal than their attachment on the next lower rib and thus lower the thorax during contraction.
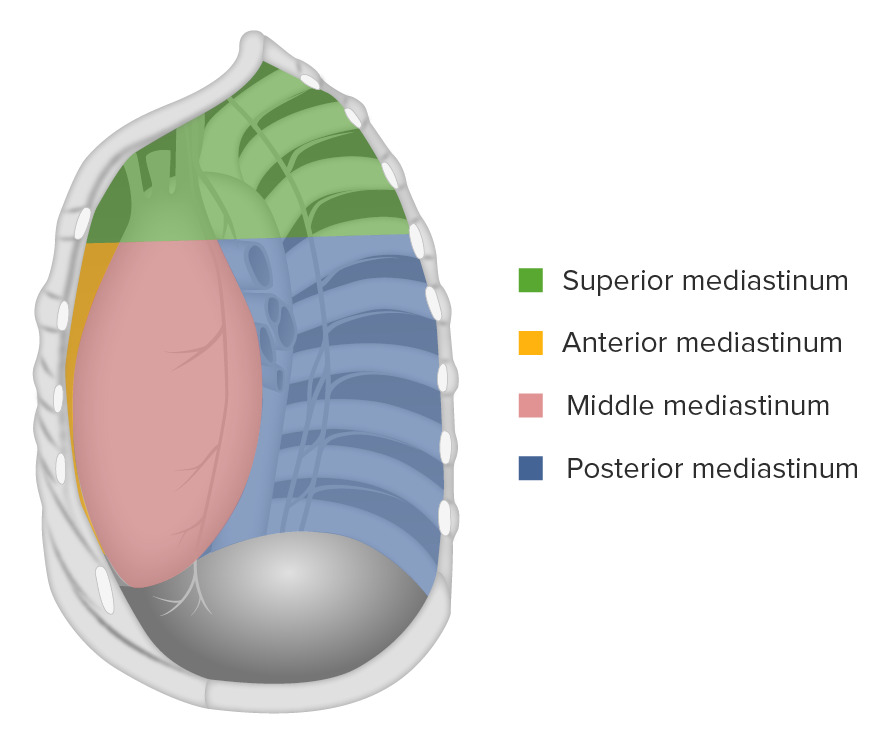
- They have their origin more ventral and distal than their attachment to the next higher rib and thus lower the thorax during contraction.
- They bring the ribs together, thus narrowing the intercostal space and lowering the thorax.
- They form a seal in the thorax.
With respect to the primary thoracic muscles, which statement is NOT true?
- The internal intercostal muscles are inspiratory.
- The internal intercostal muscles lie between the external and innermost intercostales.
- The intercostal nerve runs in the superior portion of the intercostal space.
- Muscles that lift the sternal end of the ribs are expiratory.
- The transversus thoracis muscle originates from the costal tuberosities.
Which of the following statements is the most accurate?
- The internal thoracic artery is covered by the endothoracic fascia.
- The internal thoracic artery is called the inferior epigastric artery below the epigastric angle.
- The internal thoracic artery passes through the trigonum lumbocostale.
- The internal thoracic artery is the first branch of the brachial artery.
- The internal thoracic artery travels along the midclavicular line.
With respect to the serratus anterior muscle, which of the following statements is NOT true?
- Its pars inferior makes up the smallest portion.
- It can displace the inferior scapular angle laterally and medially.
- It originates from the first to the ninth ribs.
- Its innervation is by a nerve of the pars supraclavicularis of the brachial plexus.
- It is located ventral to the subscapularis muscle.
Which of the following statements is the most accurate?
- The brachiocephalic veins carry venous outflow from the mediastinum and parts of the abdominal wall.
- The lymphatic duct drains into the internal jugular vein.
- The two brachiocephalic veins are approximately equal in length.
- The thoracic duct drains into the superior vena cava.
- The brachiocephalic veins each have two venous tributaries.
With respect to the arcuate line, which statement is NOT true?
- Below the linea alba, the rectus abdominis muscle is separated from the abdominal cavity by the aponeurosis of the transversus abdominis muscle.
- The arcuate line is located at the level of the umbilicus.
- Below the linea alba, the aponeuroses of the lateral abdominal muscles run ventrally to the rectus abdominis muscle.
- Above the arcuate line, the posterior rectus sheath is formed by the aponeuroses of the transversus abdominis and internal oblique muscles.
- Above the arcuate line, the anterior part of the rectus sheath is formed by the aponeuroses of the obliquus externus abdominis muscle, as well as the obliquus internus abdominis muscle.
With respect to the course of the inferior epigastric artery, which statement is NOT true?
- It runs ventrally to the rectus abdominis muscle.
- It runs in the lateral umbilical plica.
- It is a branch of the external iliac artery.
- It originates below the inguinal ligament.
- It forms an anastomosis with the obturator artery.
When discussing the abdominal muscles, which statement is the most accurate?
- The obliquus internus abdominis muscle originates from the lower six ribs.
- The internal oblique muscle is not involved in the formation of the inguinal ligament.
- All fibers of the internal oblique abdominis muscle run orthogonally to the fibers of the external abdominal oblique muscle.
- The transversus abdominis muscle is not involved in an abdominal crunch.
- Below the inguinal ligament, the internal abdominal oblique and transversus abdominis muscles are particularly well developed.
Author of lecture Thorax and Abdominal Wall Anatomy

Prof. Dr. med. Steffen-Boris Wirth (EN)
Customer reviews
1,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
Terrible! See my review on the first video. Its so boring and badly taught. Even clicking it tires you out. He tries to make it clear but he's failing.
